Conventional tumor-centered imaging criteria, such as RECIST or Choi criteria—which incorporate both tumor size and attenuation changes to better reflect treatment-induced necrosis—do not always reflect pathological response or true biological activity, especially in the era of immunotherapy.
In our study, we explored a novel concept: evaluating treatment response through changes in the tumor-bearing renal artery rather than focusing solely on the tumor itself. We hypothesized that systemic therapy induces hemodynamic and structural changes in tumor-feeding arteries, which may better capture the biological impact of treatment.
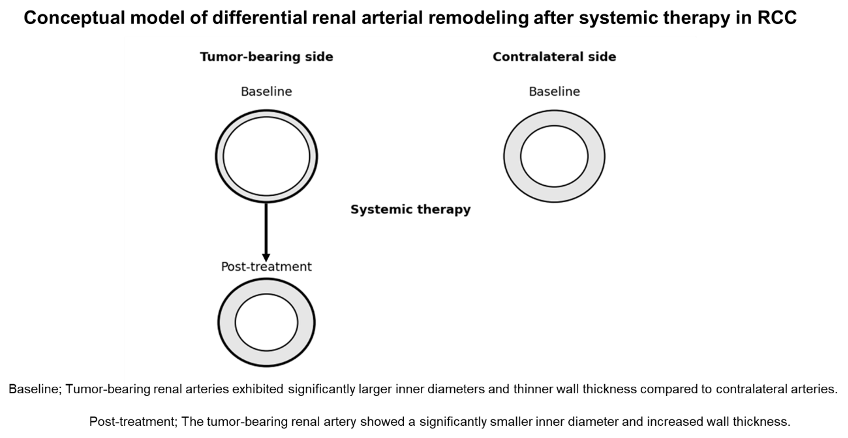
We measured renal artery caliber using curved planar reformation (CPR), a technique implemented in commercially available software widely used in clinical practice, which reconstructs vessels along their centerline to enable accurate, perpendicular cross-sectional measurement. We found that the renal artery supplying the tumor-bearing kidney was significantly dilated at baseline compared to the contralateral side, likely reflecting increased downstream blood flow demand. Following systemic therapy, this artery demonstrated a significant reduction in caliber, and importantly, the degree of reduction correlated with pathological response and downstaging. In contrast, conventional radiologic metrics did not show a significant association with pathological downstaging in our cohort.
These findings suggest that vascular changes may provide complementary information beyond tumor size or attenuation. From a clinical perspective, this approach may be particularly valuable in situations where conventional imaging yields equivocal results. For example, marked arterial narrowing could support continuation of the current therapy and consideration of surgery, whereas minimal change may prompt reassessment of treatment strategy.
The concept of evaluating upstream vascular remodeling offers a different lens through which to interpret treatment response. Rather than asking how much the tumor has shrunk, this approach asks how the tumor’s physiological environment has changed. This may be especially relevant in hypervascular tumors such as RCC, where angiogenesis plays a central role in tumor biology.
Nevertheless, several limitations must be acknowledged. This was a retrospective, single-center study with a relatively small sample size and heterogeneous treatment regimens. In addition, imaging protocols were not fully standardized, and mechanistic interpretation remains speculative, as histological evaluation of the main renal artery was not performed. Therefore, these findings should be considered hypothesis-generating and require validation in prospective, multicenter studies.
In conclusion, our study highlights the potential value of shifting from a tumor-centered to a vascular-centered perspective in response assessment. While preliminary, this approach may help bridge the gap between radiologic findings and pathological outcomes, ultimately supporting more informed clinical decision-making in patients with advanced RCC.
Written by: Himawari Asanuma,1 Teppei Okamoto,1 Tadashi Yoshizawa,2 Takuya Oishi,1 Tomoko Hamaya,1 Hirotake Kodama,1 Takuma Narita,1 Jotaro Mikami,1 Naoki Fujita,1 Tohru Yoneyama,3 Hayato Yamamoto,1 Atsushi Imai,1 Chikara Ohyama,4 Shingo Hatakeyama,1
- Department of Urology, Hirosaki University School of Medicine, 5 Zaifu-cho, Hirosaki, Aomori, Japan.
- Department of Anatomic Pathology, Hirosaki University School of Medicine, Zaifu-cho, Hirosaki, Aomori, Japan.
- Department of Glycotechnology, Hirosaki University Graduate School of Medicine, Zaifu-cho, Hirosaki, Aomori, Japan.
- Department of Advanced Transplant and Regenerative Medicine, Hirosaki University Graduate School of Medicine, Zaifu-cho, Hirosaki, Aomori, Japan.