Despite this advantage, a substantial proportion of patients will eventually relapse. As adjuvant immunotherapy becomes integrated into routine practice, the next clinical challenge is the management of recurrence after prior exposure to immune checkpoint inhibitors (ICIs).
In our retrospective single-center study, we evaluated 70 patients with high-risk RCC treated with adjuvant immunotherapy following radical nephrectomy. This cohort largely reflected the actual clinical practice, with the majority receiving pembrolizumab (71%) and a smaller proportion treated with nivolumab-ipilimumab (16%) or nivolumab monotherapy (13%). Most patients belonged to the intermediate-high risk group according to KEYNOTE-564 criteria (84%), while only 6% was high-risk, and a 10% started adjuvant therapy after radical metastasectomy (M1 NED).
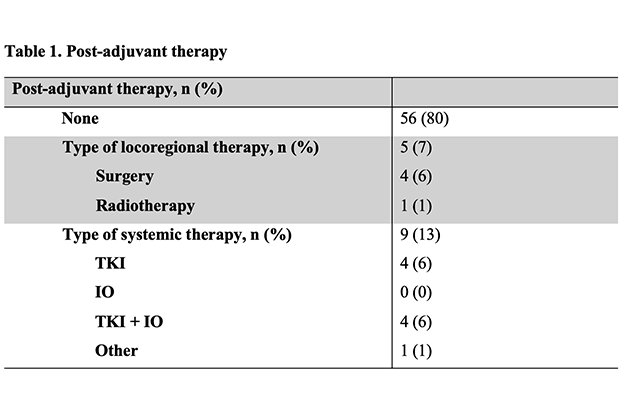
After a median follow-up of 30.2 months (26.8 – 33.6 months), 8 patients (11%) had disease recurrence after the end of adjuvant immunotherapy and 7 (10%) during adjuvant immunotherapy.
The management of patients’ disease recurrence is shown in Table 1.
The 30-month DFS rate was 74%, and the 30-month OS was 94%, consistently with the results reported in the pivotal trial.1,2 For patients with a DFS event, after a median follow-up of 24.5 months, the 24-months OS2 rate, defined as the overall survival from disease progression during or after adjuvant ICI to death or the last follow-up, was 100% for those who received a local treatment and 86% for those who received systemic treatment.
To our knowledge, only one study has specifically addressed the rate, features, and clinical management of disease recurrence after adjuvant immunotherapy in RCC, making this topic of interest for clinicians involved in RCC treatment.3
In the management of these patients, some key factors are important to consider, including the time to disease recurrence after adjuvant therapy and the disease burden (oligo- vs. poly-metastatic patients). Oligometastatic disease is generally associated with a better prognosis and may benefit from loco-regional therapeutic approaches.4
Although interpretation must be cautious due to the limited sample size and the inherent biological differences between oligometastatic and disseminated disease, our findings suggest that, in carefully selected cases, metastasis-directed therapy may provide durable disease control without immediate exposure to systemic agents.
The early use of ICIs in the adjuvant setting has also generated uncertainty regarding optimal systemic therapy at relapse. Whether patients progressing after adjuvant immunotherapy should receive immunotherapy-based combinations again remains a matter of debate. Recent randomized trials in previously treated metastatic RCC have failed to demonstrate a clear benefit for immunotherapy re-challenge over VEGFR–TKI monotherapy.5,6 In this context, VEGFR–TKI–based regimens currently represent a rational backbone for many patients relapsing after adjuvant immunotherapy.
Our data are consistent with these findings, supporting a personalized approach in which treatment selection after adjuvant immunotherapy should consider different key factors, such as timing, pattern of recurrence, size, site, as well as the risk and biological profile. Suggested management of disease recurrence after adjuvant immunotherapy is shown in Figure 1.
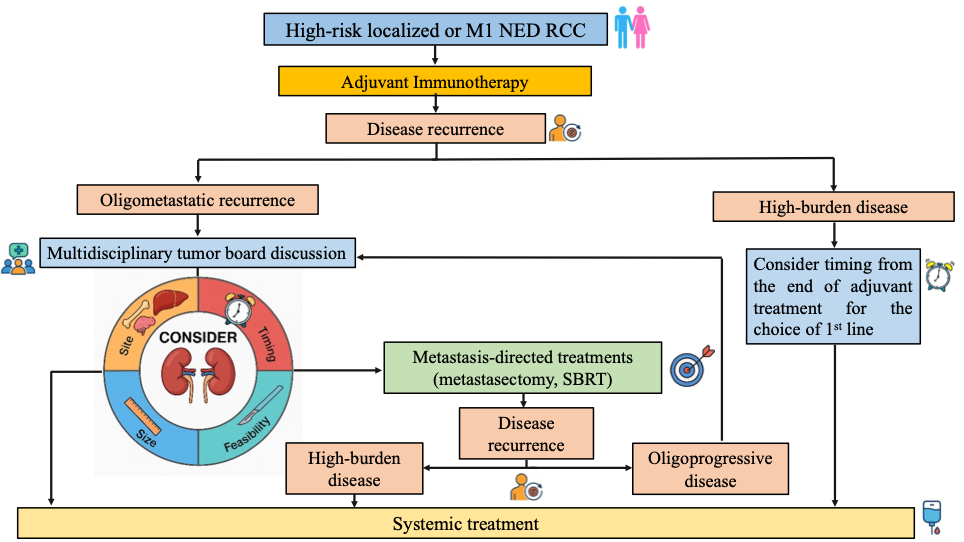
Figure 1. Suggested Management of Disease Recurrence After Adjuvant Immunotherapy
The optimal management of recurrence after adjuvant immunotherapy, therefore, requires a multidisciplinary approach, which considers all these features. In selected individuals with limited metastatic burden, metastasis-directed strategies such as stereotactic radiotherapy or surgical resection can delay systemic treatment, preserve quality of life, and potentially maintain long-term disease control. Careful patient selection is essential, and decisions should involve close collaboration among medical oncologists, urologists, and radiation oncologists.
As adjuvant immunotherapy becomes increasingly adopted worldwide, defining the best management after recurrence is one of the most debated questions in RCC. Future research should focus on identifying biomarkers that predict relapse risk and recurrence pattern, clarifying the role of immunotherapy re-challenge, and prospectively evaluating metastasis-directed strategies in this unique setting.
In conclusion, high-risk RCC patients treated with adjuvant immunotherapy remain at meaningful risk of relapse. When a systemic treatment is required, VEGFR–TKI–based regimens seem to be the preferred option; however, in selected patients, a loco-regional strategy may achieve high post-progression outcomes without immediate need for systemic therapy, thus requiring a multidisciplinary approach.
Written by: Denis Occhipinti,1 Chiara Ciccarese,1,2 and Roberto Iacovelli1,2
- Department of Translational Medicine and Surgery, Università Cattolica del Sacro Cuore, Rome, Italy.
- Medical Oncology, Department of Medical and Surgical Sciences, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy.
- Choueiri TK, Tomczak P, Spark SH, et al. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N Engl J Med 2021; 385: 683-694.
- Choueiri TK, Tomczak P, Spark SH, et al. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med, 2024; 390: 1359-1371.
- El Zarif T, Semaan K, Xie W, et al. First-line Systemic Therapy Following Adjuvant Immunotherapy in Renal Cell Carcinoma: An International Multicenter Study. Eur Urol 2024; 86(6):503-512.
- Guckenberger M, Lievens Y, Bouma AB, et al. Characterisation and classification of oligometastatic disease: A European Society for Radiotherapy and Oncology and European Organisation for Research and Treatment of Cancer consensus recommendation. Lancet Oncol 2020; 21: e18–e28.
- Pal SK, Albiges L, Tomczak P, et al. Atezolizumab plus cabozantinib versus cabozantinib monotherapy for patients with renal cell carcinoma after progression with previous immune checkpoint inhibitor treatment (CONTACT-03): a multicentre, randomised, open-label, phase 3 trial. The Lancet 2023; 402(10397):185–95.
- Choueiri TK, Albiges L, Barthélémy P, et al. Tivozanib plus nivolumab versus tivozanib monotherapy in patients with renal cell carcinoma following an immune checkpoint inhibitor: results of the phase 3 TiNivo-2 Study. Lancet 2024; 404(10460):1309–20.