
Figure 1: Glycosaminoglycans (GAGs) are long, unbranched polysaccharides located in the extracellular matrix and on cell surfaces, indicated to play key roles in cell signaling, tumor microenvironment integrity, and immune evasion.
The GAGome represents the specific profile of GAG molecules detected in biological fluids (e.g., urine) by UHPLC-MS/MS. The GAGome score is a composite biomarker (0–100) derived from a mathematical model applied to measured GAGomes, correlating with recurrence probability in ccRCC. Abbreviations: ccRCC = clear cell Renal Cell Carcinoma. GAG = Glycosaminoglycan; GAGome = GAG profile; NED = No evidence of disease; RD = Recurrent disease; UHPLC-MS/MS = Ultra-high-performance liquid chromatography–tandem mass spectrometry.
The AURORAX-0087A study is a prospective, multicentre study composed of two sequential cohorts and designed to evaluate whether the urine-based GAGome score can provide recurrence risk information during surveillance and offer additional prognostic value in patients curatively treated for localised ccRCC. Cohort 1, recently published in European Urology Oncology, enrolled 134 patients from 23 centres. Radiological recurrence was confirmed in 21 (16%) patients during the study period. Compared to standard-of-care imaging-based surveillance, the observed GAGome score sensitivity and negative predictive value estimates for ccRCC recurrence detection were 90% and 97% respectively, with a median 4.2-month lead time over imaging. Additionally, each 10-point increase of the GAGome score was associated with a 62% higher recurrence risk.5 These exploratory findings indicate that elevated GAGome scores may correlate with biochemical changes observed in patients who later recurred, a hypothesis that requires further validation.
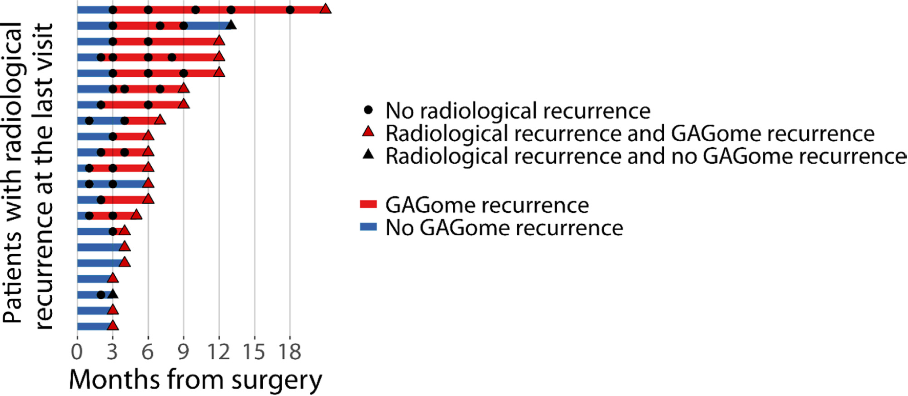
Figure 2 (adapted from Dabestani et al5: Swimmer plot for the 21 patients with radiological recurrence during follow-up, where each bar represents a patient and each point a follow-up visit with radiological assessment (circle: no radiological recurrence assessed; triangle: radiological recurrence assessed). GAGome recurrence is defined as a GAGome score higher than the cut-off (>12%) and no GAGome recurrence otherwise. The blue portion of each bar indicates the time during which no GAGome recurrence was assessed in the underlying sample collection visits (note that these are more frequent than follow-up visits with radiological assessment). The red portion represents the time during which GAGome recurrence was assessed in the underlying sample collection visits. If GAGome recurrence was assessed at the same time as radiological recurrence was assessed (thus ending the study for that patient), the corresponding triangle point is coloured in red, otherwise in black. Note that in five patients, the first visit in which GAGome recurrence was assessed is the same visit in which radiological recurrence was assessed (lead time = 0 d), so no red portion of the bar is shown. GAGome = glycosaminoglycan profile.
In this explorative study, negative test results were rarely followed by radiologic evidence of recurrence, while positive tests were more often observed in patients who subsequently experienced recurrence. These findings, if validated, suggest that for ccRCC patients, the test may inform about how to refine postoperative surveillance strategies when interpreted alongside clinical assessment and imaging results.
Pending successful external validation in Cohort 2 (140 patients) of AURORAX-0087A (for which the last patient's last visit was reached in May of 2025), the GAGome score may provide a non-invasive means to support individualised RCC surveillance. Its integration with existing risk models may, in the future, help tailor follow-up intensity, pending demonstration of safety and clinical utility.
Future Perspectives
Unanswered questions remain. First, can GAGome score improve upon or integrate with the Leibovich score for ccRCC? The rationale is that whereas Leibovich reflects static pathology, GAGomes are suggested to capture real-time tumour metabolism.6,7 Whether this improves risk discrimination is a key endpoint of long-term follow-up of future studies, in particular for low-risk ccRCC. Ancillary to this, a hypothesis to be tested lies in assessing whether equivocal lesions detected on standard-of-care imaging during follow-up for ccRCC recurrence (e.g., lung lesions) can be more accurately classified as true recurrence or benign findings using the GAGome score measured at the time of radiological evaluation. Second, adjuvant systemic therapy has emerged as a new standard of care offered to patients with intermediate-high to high-risk ccRCC (with pembrolizumab currently the only approved treatment). While such treatment offers survival benefits, concerns remain regarding overtreatment, toxicity, and the absence of reliable biomarkers to guide patient selection.8 In this context, a post-nephrectomy GAGome score indicating minimal residual disease could help clearly identify patients for adjuvant therapy, while a non-elevated score may exclude those unlikely to need it. Lastly, the potential utility of GAGomes as diagnostic and prognostic tools in non-ccRCC subtypes, as well as in the metastatic setting to guide systemic treatment decisions, remains to be explored.
The GAGome test is being developed by Elypta AB, a Swedish diagnostics company, is investigational and currently not approved for clinical use. Elypta AB sponsors the AURORAX-0087A study and is co-funded by the European Union Horizon 2020 programme (Grant No. 849251)
Written by: Saeed Dabestani,1 Nessn H Azawi,2 Riccardo Campi,3 Petrus Järvinen,4 Harry Nisen,4 Umberto Capitanio,5 Tommy Kjærgaard Nielsen,6 Giuseppe Simone,7 Mark Rochester,8 Euan Green,9 Sergio Fernandez-Pello,10 Christopher Blick,11 Francesco Porpiglia,12 Alexandre Ingels,13 Sinisa Bratulic,14 Alessandro Antonelli,15 A Ari Hakimi,16 Michael A S Jewett,17 Börje Ljungberg,18 Bimal Bhindi,19 Lorenzo Marconi,20 Alexander Laird,21 Grant D Stewart,22 Rajesh Nair,23 Lars Lund,24 Neil Barber,25 Viraj A Master,26 Andrea Minervini,27 Jose A Karam,28 Francesco Gatto,29 Axel Bex30
- Department of Translational Medicine, Division of Urological Cancers, Lund University, Lund, Sweden; Department of Urology, Kristianstad Central Hospital, Region Skane, Kristianstad, Sweden.
- Institute of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark.
- Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy; Unit of Urological Robotic Surgery and Renal Transplantation, Careggi Hospital, Florence, Italy.
- Department of Urology, Helsinki University Hospital, Helsinki, Finland.
- IRCCS San Raffaele Scientific Institute, Urological Research Institute (URI), Milan, Italy.
- Department of Urology, Aalborg University Hospital, Aalborg, Denmark; Department of Clinical Medicine, Aalborg University, Aalborg, Denmark.
- Department of Urology, IRCCS "Regina Elena" National Cancer Institute, Rome, Italy.
- Department of Urology, Norfolk & Norwich University Hospital, Norwich, UK; Norwich Medical School, UEA, Norwich, UK.
- Department of Urology, Salford Royal Hospital, Northern Care Alliance, Salford, UK.
- Department of Urology, Cabueñes University Hospital, Gijón, Spain.
- Harold Hopkins Department of Urology, Royal Berkshire Hospital, Reading, UK.
- Department of Oncology, Division of Urology, University of Turin, San Luigi Gonzaga Hospital, Turin, Italy.
- Department of Urology, Henri Mondor Hospital, University of Paris Est Créteil (UPEC), Créteil, France; Biomaps, UMR1281, INSERM, Centre National de la Recherche Scientifique (CNRS), Commissariat à l'Energie, Créteil, France.
- Elypta AB, Stockholm, Sweden.
- Department of Urology, AOUI Verona, University of Verona, Verona, Italy.
- Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
- Departments of Surgery and Surgical Oncology, Division of Urology, Princess Margaret Cancer Centre, University Health Network and the University of Toronto, Toronto, Ontario, Canada.
- Department of Diagnostics and Intervention, Urology and Andrology, Umeå University, Umeå, Sweden.
- Department of Surgery, Section of Urology, University of Calgary, Calgary, Alberta, Canada.
- Department of Urology, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal; Faculty of Medicine, University of Coimbra, Coimbra, Portugal.
- Institute of Genetics and Cancer, The University of Edinburgh, Western General Hospital. Edinburgh, UK; Department of Urology, Western General Hospital, Edinburgh, UK.
- Department of Surgery, University of Cambridge, Cambridge Biomedical Campus, Cambridge, UK; CRUK Cambridge Centre, Cambridge Biomedical Campus, Cambridge, UK.
- The Urology Centre, Guy's and St. Thomas' NHS Foundation Trust, Guy's Hospital, London, UK.
- Department of Urology, Odense University Hospital, Odense, Denmark; Department of Clinical Research, University of Southern Denmark, Odense, Denmark.
- Department of Urology, Frimley Health NHS Foundation Trust, Frimley, UK.
- Department of Urology, Winship Cancer Institute, Emory University, Atlanta, GA, USA.
- Department of Experimental and Clinical Medicine, University of Florence, Florence Italy; Unit of Oncologic Minimally-Invasive Urology and Andrology, Careggi Hospital, University of Florence, Florence, Italy.
- Department of Urology and Department of Translational Molecular Pathology, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
- Department of Translational Medicine, Division of Urological Cancers, Lund University, Lund, Sweden; Elypta AB, Stockholm, Sweden.
- Department of Urology, The Royal Free London NHS Foundation Trust, London, UK; Division of Surgery and Interventional Science, University College London, London, UK; Department of Urology, Netherlands Cancer Institute, Amsterdam, The Netherlands.
- Dabestani S, Thorstenson A, Lindblad P, Harmenberg U, Ljungberg B, Lundstam S. Renal cell carcinoma recurrences and metastases in primary non-metastatic patients: a population-based study. World J Urol. 2016.
- Bedke J, Ghanem YA, Albiges L, Bonn S, Campi R, Capitanio U, et al. Updated European Association of Urology Guidelines on the Use of Adjuvant Immune Checkpoint Inhibitors and Subsequent Therapy for Renal Cell Carcinoma. European Urology. 2025;87(4):491-6.
- Iisager L, Ahrenfeldt J, Keller AK, Nielsen TK, Fristrup N, Lyskjær I. KIDNEY-PAGER: analysis of circulating tumor DNA as a biomarker in renal cancer - an observational trial. Study protocol. Acta Oncol. 2024;63:51-5.
- Gatto F, Dabestani S, Bratulic S, Limeta A, Maccari F, Galeotti F, et al. Plasma and Urine Free Glycosaminoglycans as Monitoring Biomarkers in Nonmetastatic Renal Cell Carcinoma-A Prospective Cohort Study. Eur Urol Open Sci. 2022;42:30-9.
- Dabestani S, Azawi NH, Campi R, Järvinen P, Nisen H, Capitanio U, et al. Urine Glycosaminoglycan Scores for Surveillance of Recurrence in Intermediate- and High-risk Nonmetastatic Clear Cell Renal Cell Carcinoma-An Observational Prospective Multicentre Diagnostic Test Cohort Study. Eur Urol Oncol. 2025.
- Calhoon D, Sang L, Ji F, Bezwada D, Hsu SC, Cai F, et al. Glycosaminoglycan-driven lipoprotein uptake protects tumours from ferroptosis. Nature. 2025;644(8077):799-808.
- Bratulic S, Limeta A, Dabestani S, Birgisson H, Enblad G, Stalberg K, et al. Noninvasive detection of any-stage cancer using free glycosaminoglycans. Proceedings of the National Academy of Sciences of the United States of America. 2022;119(50):e2115328119.
- Marandino L, Campi R, Amparore D, Tippu Z, Albiges L, Capitanio U, et al. Neoadjuvant and Adjuvant Immune-based Approach for Renal Cell Carcinoma: Pros, Cons, and Future Directions. Eur Urol Oncol. 2025;8(2):494-509.