Management of metastatic ccRCC has evolved with the approval of immune checkpoint inhibitors (ICIs), often combined with tyrosine kinase inhibitors (TKIs). However, nccRCC treatments still rely primarily on VEGF-targeting TKIs, due to limited high-level evidence supporting ICIs in this setting. Some phase II trials (e.g., KEYNOTE-427, CheckMate 374, and SUNNIFORECAST) and retrospective studies have suggested promising outcomes using ICI-based therapies for nccRCC. These findings have yet to be fully validated in real-world, multicenter data, hence the rationale for the ARON-1 study.
The ARON-1 study is a large international, retrospective analysis of real-world data from patients with metastatic nccRCC treated with first-line immune-based combination therapies between January 2021 and December 2024. The data were collected from 56 centers in 17 countries, with a focus on intermediate- and poor-risk patients according to the IMDC risk model.
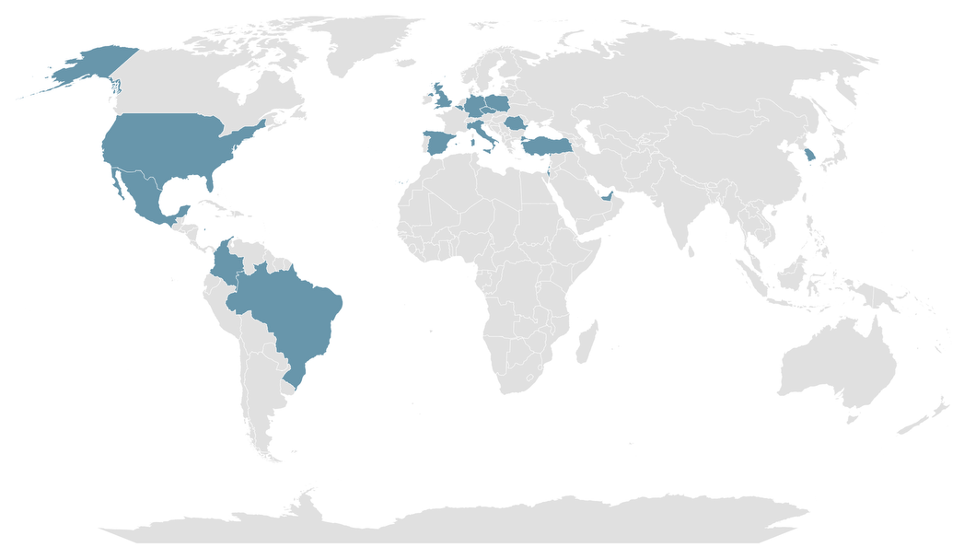
Figure 1. Map of participating Countries in the ARON-1 study.
Eligible patients had histologically confirmed nccRCC, measurable metastatic disease, and had received at least one cycle of an ICI-based first-line therapy. Patients were excluded if they lacked tumor response data or follow-up. The primary endpoints were overall survival (OS) and progression-free survival (PFS), evaluated using RECIST 1.1 criteria. Secondary outcomes included objective response rate (ORR) and safety.
Statistical analyses included Kaplan-Meier survival curves, Cox regression models, and comparisons among different ICI-based combinations (e.g., nivolumab/ipilimumab, pembrolizumab/axitinib, pembrolizumab/lenvatinib, and nivolumab/cabozantinib).
Out of 2,401 patients in the ARON-1 dataset treated with immune combinations, 323 had nccRCC and were included in this analysis. The median age was 63 years; 75% were male.
Histologic subtypes included:
- Papillary RCC (46%)
- Chromophobe RCC (11%)
- Other/rare nccRCC (43%)
First-line immune-based combinations included:
- Pembrolizumab/axitinib (34%)
- Nivolumab/ipilimumab (31%)
- Nivolumab/cabozantinib (23%)
- Pembrolizumab/lenvatinib (12%)
- Median OS (mOS) in the overall population was 31.1 months with a 2-year OS rate of 58%.
- Patients who had undergone nephrectomy had significantly longer OS (40.4 vs. 19.9 months).
- Intermediate-risk patients had mOS of 36.1 months compared to 11.9 months for poor-risk patients.
- OS was significantly worse for patients with bone or liver metastases.
- Pembrolizumab/lenvatinib: mOS 31.9 months; 2-year OS: 69%
- Pembrolizumab/axitinib: mOS 31.2 months; 2-year OS: 61%
- Nivolumab/cabozantinib: mOS 27.8 months; 2-year OS: 54%
- Nivolumab/ipilimumab: mOS 24.6 months; 2-year OS: 51%
- pRCC patients benefited most from pembrolizumab/lenvatinib (2-year OS 77%)
- chRCC patients showed best OS with pembrolizumab/axitinib (mOS 40.5 months)
- uRCC patients had variable results, with nivolumab-based therapies showing potential benefit

Figure 2. Overall Survival in metastatic nccRCC patients receiving first-line immune-base combinations, stratified by clinical features.
Progression-Free Survival (PFS)
Median PFS across the entire cohort was 13.0 months, with a 1-year PFS rate of 52%.
PFS by treatment:
- Pembrolizumab/lenvatinib: 24.5 months, 1-year PFS: 66%
- Nivolumab/cabozantinib: 18.4 months, 1-year PFS: 63%
- Pembrolizumab/axitinib: 13.4 months, 1-year PFS: 57%
- Nivolumab/ipilimumab: 6.8 months (shortest), 1-year PFS: 35%
Among patients with pRCC, pembrolizumab/lenvatinib showed the highest 1-year PFS (73%).

Figure 3. Overall Survival and Progression-Free Survival in metastatic nccRCC patients stratified by type of first-line immune-based combination.
Objective Response Rate (ORR)
The overall ORR was 38%, with 2% achieving complete response (CR) and 36% partial response (PR).
ORRs by treatment:
- Pembrolizumab/lenvatinib: 59% (highest), with 5% CR
- Nivolumab/cabozantinib: 40%
- Pembrolizumab/axitinib: 35%
- Nivolumab/ipilimumab: 32%
In the poor-risk subgroup, pembrolizumab/lenvatinib also achieved the highest ORR (49%) but sample size was small.
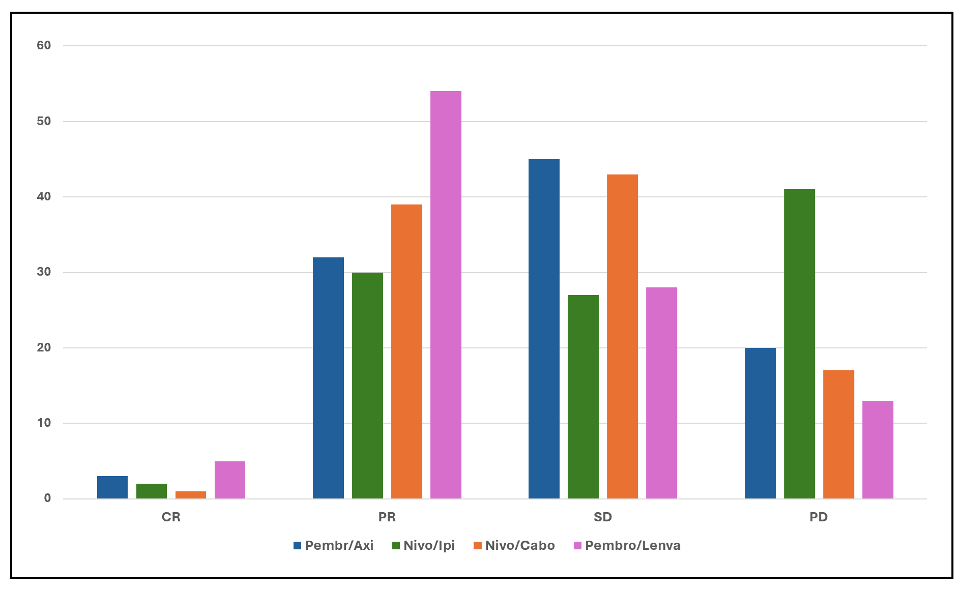
Figure 4. Response to first-line immune-based combinations in patients with advanced nccRCC.
This study represents the largest real-world multicenter dataset assessing ICI-based therapies in intermediate-/poor-risk nccRCC patients. Results confirm that ICI/TKI combinations are more effective than ICI-doublets, supporting their role as preferred first-line options.
Among all regimens:
- Pembrolizumab/lenvatinib was associated with the highest ORR (59%), longest PFS (24.5 months), and best 2-year OS (69%), aligning well with findings from the KEYNOTE-B61 trial.
- Pembrolizumab/axitinib was widely used and showed favorable outcomes, especially in pRCC and chRCC, although prospective data for this combination in nccRCC are lacking.
- Nivolumab/cabozantinib performed well in chRCC and uRCC, despite the chRCC cohort being discontinued early in a previous trial due to lack of benefit.
- Nivolumab/ipilimumab, although included in standard care for ccRCC, had relatively lower effectiveness in nccRCC, especially in terms of PFS and ORR.
Written by: Veronica Mollica,1 Francesco Massari,1,2 Matteo Santoni3
- Medical Oncology, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy;
- Department of Medical and Surgical Sciences (DIMEC), University of Bologna, Bologna, Italy;
- Medical Oncology Unit, Macerata Hospital, Macerata, Italy.