CH is also a major confounder of plasma-only blood-based cell-free DNA (cfDNA) companion diagnostic tests that don’t profile matched leukocytes because the majority of plasma cfDNA originates from degrading hematopoietic cells. The prevalence of CH in metastatic renal cell (mRCC) and urothelial carcinoma (mUC) and the degree to which it confounds liquid biopsy tests used in the management of genitourinary cancers are unknown.
To address this gap, we obtained blood samples from 299 patients with mRCC or mUC through our provincial biobank and applied our custom ultra-deep error-corrected targeted DNA sequencing assay to both cfDNA and leukocyte DNA for CH detection. This dual-source approach was a major strength of our study that allowed us to confidently distinguish CH from tumor-derived mutations.
Two of the questions we explored were:
- What are the prevalence and characteristics of CH in mRCC and mUC?
- What is the potential for CH to confound blood-based liquid biopsy tests that don’t incorporate patient-matched controls, and how can this issue be mitigated?
We observed that genes with established relevance in solid tumors carried CH and tumor-originating mutations at a similar prevalence: 91%, 70%, 27% and 32% of all detected mutations in CHEK2, ATM, BRCA2 and TP53 respectively originated from CH, as well as 33% of mutations in ERBB2, a candidate biomarker for anti-HER2 antibody-drug conjugate therapy in mUC (Figure 1). These findings have direct clinical implications. Without patient-matched controls, these mutations are at risk of being misclassified as tumor-derived. False positives due to CH may not only lead to improper treatment allocation, but also may falsely imply nonzero tumor fraction in the absence of any other tumor-originating mutation. This could lead to the erroneous interpretation of negative tumor mutation status for all other reported genes and potentially preclude follow-up tissue genotyping.
Patient-matched leukocyte sequencing is the gold standard to rule out CH. When both cfDNA and leukocyte DNA are sequenced, false positives due to CH can be excluded on the basis of detection in both specimens, while tumor-derived mutations are typically present in cfDNA only. Our computer simulation experiments suggest sequencing the leukocyte DNA to 25% of cfDNA sequencing depth is a cost-effective solution that is capable of detecting 90% of the CH mutations with allelic frequency >1%.
In conclusion, our study provides the first comprehensive characterization of CH in metastatic urinary malignancies and supports the incorporation of matched leukocyte DNA sequencing into blood-based liquid biopsy companion diagnostic tests to ensure accuracy. We also emphasize the invaluable role of biobanks in greatly accelerating cancer research; this study wouldn’t be possible without the generosity of patients who donated blood to our provincial Genitourinary Cancer Biobank in British Columbia.
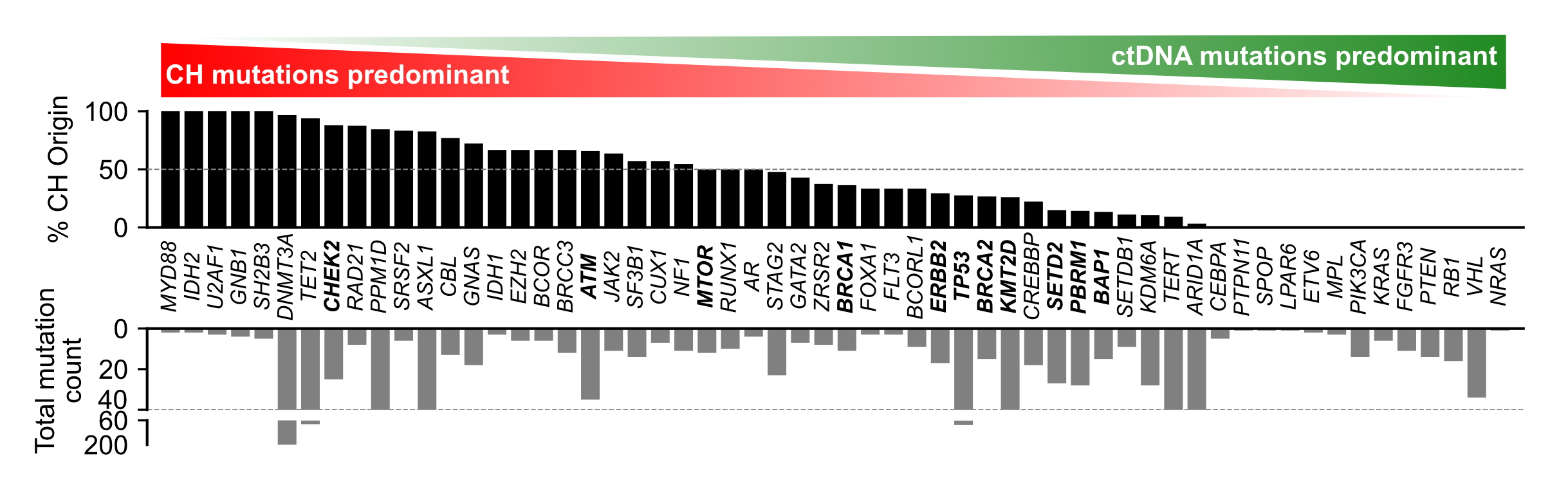
Caption for Figure 1: Percentage of all somatic mutations detected in cfDNA that are CH-derived, shown on a per-gene basis.
Written by: Aslı D. Munzur,1 Jack V. W. Bacon,1 Francine Fishbein,2 Cameron Herberts,1 Gráinne Donnellan,1 Cecily Q. Bernales,1 Karan Parekh,1 Gillian Vandekerkhove,1,3 David C. Müller,1,4 Yi Jou Ruby Liao,1 Maria Stephenson,1 Lucia Nappi,1,3 Daniel Khalaf,3 Corinne Maurice-Dror,3 Kim N. Chi,1,3 Bernhard J. Eigl,1,3 Christian Kollmannsberger,1,3 Maryam Soleimani,3 Alexander W. Wyatt1,5
- Vancouver Prostate Centre, Department of Urologic Sciences, University of British Columbia, Vancouver, BC, Canada
- Department of Internal Medicine, University of British Columbia, Vancouver, BC, Canada
- Department of Medical Oncology, BC Cancer, Vancouver, BC, Canada
- Department of Urology, University Hospital Basel, University of Basel, Basel, Switzerland
- Clinical Cancer Genomics Program and Michael Smith Genome Sciences Centre, BC Cancer, Vancouver, BC, Canada