However, recent evidence suggests that AS may also be appropriate in selected younger individuals with low-risk tumors. As AS is increasingly considered a long-term strategy, the safety of repeated imaging — particularly with CT and accumulated radiation dose — becomes an important concern.
This study was a joint effort between the Department of Radiology and Urology at Akershus University Hospital. It was initially inspired by our experience in monitoring iceball expansion during CT-guided cryoablation of renal tumors. In that context, we observed that key tumor metrics — such as size and location — could be reliably assessed even at substantially reduced CT dose levels. That observation led us to ask whether the same might apply in the context of AS imaging, where precise and reproducible size measurements are essential for guiding clinical decisions.
We conducted a multi-observer study with the participation of nine radiologist observers from Akershus University Hospital in Norway, Aarhus University Hospital, and Aalborg University Hospital in Denmark. The observers evaluated routine-dose contrast-enhanced CT against simulated lower-dose datasets, both with and without the application of a commercially available deep learning–based denoising (DLD) algorithm, which operates at the DICOM image level and is CT vendor-neutral. Using CT data from 70 patients with SRMs, we used a validated technique to synthetically generate reduced dose levels of 75% and 90% and then reconstructed images with and without DLD. The radiologists independently reviewed these datasets for image quality and renal mass assessment, including size, nearness to the collecting system, and shape irregularity.
Our results demonstrated that even with a 75% dose reduction using conventional interactive reconstruction, diagnostic performance remained intact. When DLD was applied, image quality improved significantly, and the consistency of scan assessments was preserved. Especially tumor size assessments—the key metric for monitoring progression in active surveillance—remained reproducible across dose levels, except at a 90% dose reduction using iterative reconstruction. However, when applying DLD, reproducibility at this ultra-low-dose level was similar to that observed at routine dose levels, as were other important morphological features like tumor shape irregularity and nearness to the collecting system. These findings suggest that safe, sub-millisievert imaging for AS is achievable on a broad scale, even on older CT hardware.
This is especially relevant in light of growing concerns about the long-term risks of medical radiation. A recent large-scale modeling study by Smith-Bindman et al. projected that CT imaging could eventually account for 5% of all new cancer diagnoses annually.1 The authors emphasized that even low-dose exposures are not without risk, and crucially, that the latency period for radiation-induced cancers typically spans one to two decades. Since the literature supporting AS of SRMs has only emerged in the past 20 years, we are only beginning to appreciate the long-term implications of repeated CT imaging, particularly in younger patients. This underlines the need to refine surveillance strategies to minimize harm while preserving diagnostic confidence in accordance with the ALARA (As Low As Reasonably Achievable) principle that guides all radiation-based medical imaging.2
Our findings offer a clear path forward: substantial dose reduction in CT-based surveillance of SRMs is achievable, even with conventional iterative reconstruction techniques, and with even greater dose reduction possible with the addition of deep learning–based denoising. For urologists managing patients in AS protocols, this underscores the value of closer collaboration with radiologists to implement safe, low-dose imaging strategies that maintain diagnostic confidence.
Looking ahead, open questions remain. What is the optimal timing of follow-up scans in AS? Can we reduce imaging frequency without compromising patient safety? What role might non-contrast abbreviated MRI protocols play, particularly in younger patients? Additionally, the potential of deep learning–based denoising in low-dose CT surveillance of urolithiasis also warrants further investigation, given the similarly recurrent imaging needs in that population. Our research group — and hopefully others — will continue to explore these pressing questions, with the goal of refining and individualizing AS imaging strategies in the years to come.
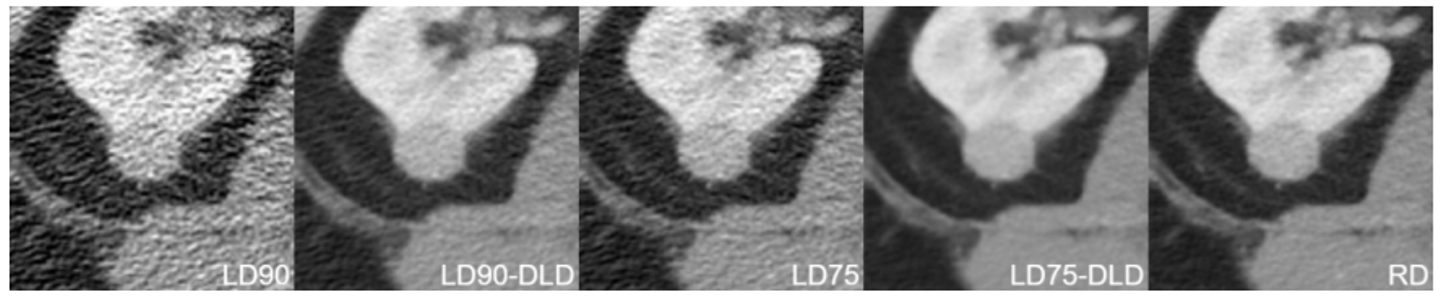
Figure 1: Contrast-enhanced axial CT images (3-mm section thickness) depicting a 2.2-cm well-circumscribed, homogeneous, exophytic small renal mass in a 70-year-old female patient at various dose levels: lower dose with 90% dose reduction (LD90); lower dose with 90% dose reduction and deep learning–based denoising (LD90-DLD); lower dose with 75% dose reduction (LD75); lower dose with 75% dose reduction and deep learning–based denoising (LD75-DLD); and routine dose (RD).
Reprinted from Borgbjerg et al., Radiology: Cancer Imaging, 2024 (https://doi.org/10.1148/rycan.240250).
Written by:
- Jens Borgbjerg, MD PhD, Department of Radiology, Akershus University Hospital, Norway
- Bendik Breen, MD, Department of Radiology, Akershus University Hospital, Norway
- Anne Negård, MD PhD, Department of Radiology, Akershus University Hospital, Norway
- Jens Brøndum Frøkjær, MD PhD, Department of Radiology, Aalborg University Hospital, Denmark
- Tommy K. NIelsen, MD PHD, Department of Urology, Aalborg University Hospital, Denmark
- Stig Müller, MD PHD, Department of Urology, Akershus University Hospital, Norway
References:
- Smith-Bindman, R. et al. Projected Lifetime Cancer Risks From Current Computed Tomography Imaging. JAMA Intern Med 185, 710–719 (2025).
- Boone, J. M., Hendee, W. R., McNitt-Gray, M. F. & Seltzer, S. E. Radiation exposure from CT scans: how to close our knowledge gaps, monitor and safeguard exposure--proceedings and recommendations of the Radiation Dose Summit, sponsored by NIBIB, February 24-25, 2011. Radiology 265, 544–554 (2012).