When the NB-GFR drops below 45ml/min/1.73m2 after renal cancer surgery, patient survival begins to decline, whereas those above this threshold have outcomes comparable to patients without CKD.1 The present study evaluates a novel artificial intelligence (AI)-based approach to predict NB-GFR following PN and RN.
The study evaluates 293 patients undergoing renal surgery (111 RN and 182 PN) with preoperative arterial-phase CT-imaging.2 The authors employ a split renal function (SRF) based approach for NB-GFR prediction following RN. Prior studies have demonstrated SRF approaches are superior to other methodologies for NB-GFR prediction, and differential parenchymal volume analysis (PVA) appears to be the best method for estimating SRF.3,4 Existing techniques for PVA include manual segmentation and semi-automated software analysis, which take approximately 30 minutes and 5 minutes to perform, respectively, and occasionally require manual exclusion of the renal pelvis, vessels, and cysts.
This study leverages a deep learning model (nnU-Net framework) to generate fully automated segmentation masks for differential PVA (Figure 1).5 The neural network was trained on approximately 50,000 manually segmented CT axial slices. Contralateral SRF estimates from the AI model were then applied to a previously validated equation for NB-GFR prediction after RN:
“NBGFR=1.24×(PreopGFR)×(SRFContra)”, where 1.24 represents the average degree of renal functional compensation in adults.4
For the prediction of NB-GFR following PN, the authors employed a simple model based on the “80/90” rule, which states that the average function saved in the operated kidney ≈80%, and if there is a contralateral kidney, the global function saved averages ≈90%.6 This results in the simple equation: “NB-GFR=PreopGFR×0.9”, and for this image analysis is not required.
The AI model predicted NB-GFR with a correlation coefficient of 0.75, comparable to a previously validated clinical model (r = 0.77).7 Notably, both models also performed equivalently in predicting whether a patient’s NB-GFR would fall below the critical threshold of 45 ml/min/1.73 m². The AI-based approach offers several potential advantages over existing models. It requires no user input, eliminating the need for manual segmentation or exclusion of renal sinus structures, unlike previous PVA methods, and thus might be more objective. Additionally, its simplicity enhances usability compared to traditional clinical models, which often involve complex multivariable algorithms that limit practicality at the point of care.
AI-driven approaches for fully automated PVA and NB-GFR prediction represent an exciting advancement in research regarding the prediction of functional outcomes following renal surgery. Further studies are needed to validate these approaches in clinical settings and compare them against current gold-standard methodologies.
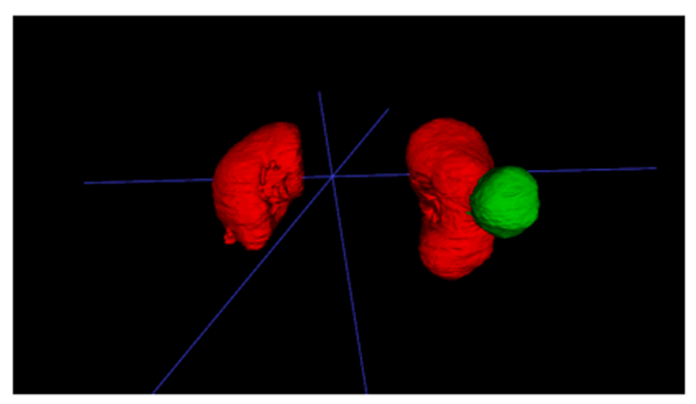
Figure 1. Example of AI-based approach for PVA and NB-GFR prediction following radical nephrectomy.
In this case, the parenchymal volumes are shown in red and directly measured by the AI software, and the contralateral SRF is estimated by contralateral volume divided by the total parenchymal volume, x 100%.
Written by: Kieran Lewis & Steven C. Campbell, MD, PhD, Department of Urology, Cleveland Clinic
Co-Authors: Nityam Rathi & Chris J. Weight, MD, Department of Urology, Cleveland Clinic
References:
- Campbell SC, Campbell JA, Munoz-Lopez C, Rathi N, Yasuda Y, Attawettayanon W. Every decade counts: a narrative review of functional recovery after partial nephrectomy. BJU Int. 2023 Feb;131(2):165–72.
- Abdallah N, Rathi N, Heller N, Wood A, Campbell R, Benidir T, et al. A Fully Automated Artificial Intelligence-Based Approach to Predict Renal Function After Radical or Partial Nephrectomy. Urology. 2025 Feb 4;S0090-4295(25)00121-9.
- Lewis K, Maina EN, Lopez CM, Rathi N, Attawettayanon W, Kazama A, et al. Limitations of Parenchymal Volume Analysis for Estimating Split Renal Function and New Baseline Glomerular Filtration Rate After Radical Nephrectomy. J Urol. 2024 Jun;211(6):775–83.
- Rathi N, Attawettayanon W, Yasuda Y, Lewis K, Roversi G, Shah S, et al. Point of care parenchymal volume analyses to estimate split renal function and predict functional outcomes after radical nephrectomy. Sci Rep. 2023 Apr 17;13(1):6225.
- Heller N, Isensee F, Maier-Hein KH, Hou X, Xie C, Li F, et al. The state of the art in kidney and kidney tumor segmentation in contrast-enhanced CT imaging: Results of the KiTS19 challenge. Med Image Anal. 2021 Jan;67:101821.
- Rathi N, Attawettayanon W, Kazama A, Yasuda Y, Munoz-Lopez C, Lewis K, et al. Practical Prediction of New Baseline Renal Function After Partial Nephrectomy. Ann Surg Oncol. 2024 Feb;31(2):1402–9.
- Aguilar Palacios D, Wilson B, Ascha M, Campbell RA, Song S, DeWitt-Foy ME, et al. New Baseline Renal Function after Radical or Partial Nephrectomy: A Simple and Accurate Predictive Model. J Urol. 2021 May;205(5):1310–20.