Treatment of renal cell carcinoma (RCC) with radical nephrectomy (RN) more frequently induces chronic kidney disease (CKD) compared to nephron-sparing surgery (NSS), which may impact overall survival. Growing awareness of the disadvantages of reduced renal function after kidney surgery has led to increased interest in the treatment of patients with T1 RCC, particularly those with tumors measuring 4 cm or smaller. It has been recognized that patients diagnosed with RCCs of 4 cm or smaller often have impaired renal function after radical nephrectomy.
In a study by Huang et al.,1 26% of patients with normal preoperative serum creatinine levels were found to have an estimated glomerular filtration rate (eGFR) below 60 ml/min/1.73 m², meeting the criteria for CKD.2 It is well established that the risk of developing or worsening CKD is significantly lower after NSS compared to RN. The progression of CKD has been linked to reduced overall survival due to an increased incidence of cardiovascular events and mortality.3
The development of nephron-sparing techniques has shifted the treatment paradigm toward partial nephrectomy (PN).3 Recent data suggest that even tumors measuring 7 cm or larger can be resected with oncological outcomes comparable to those of RN in selected cases of RCC.4,5
Based on this evidence, most current guidelines recommend NSS for stage T1 RCC when technically feasible. This recommendation is widely accepted, particularly for tumors measuring 4 cm or smaller.
Moreover, it is increasingly recognized that partial nephrectomy with tumor removal and maximal nephron preservation are underutilized in clinical practice.6 This is due to the lack of clear factors on which standardized recommendations for kidney resection in RCC should be based.
Since 2009, the urological community has been refining and enhancing two primary nephrometry systems, R.E.N.A.L and PADUA, designed to achieve two key objectives: standardizing data on kidney tumors and predicting complications.7,8 However, neither system could determine the feasibility of organ-sparing surgery. For years, the choice of surgical approach depended largely on the surgeon’s experience—what might be considered a complex case for one surgeon could be a routine partial nephrectomy for another, particularly in high-volume centers. Subsequent efforts aimed at developing a more precise classification system, though they largely adhered to the fundamental principles established by the original nephrometry models in 2009.9,10
It was hypothesized that similar to liver surgery, the remaining functional parenchymal volume (RFPV) after tumor removal could be quantified to assess the feasibility of an organ-sparing approach.11 This led to the development of a specialized formula based on CT imaging. Since 2010, this formula has been applied to all patients undergoing kidney tumor surgery in our center, providing a standardized method for evaluating the potential for nephron-sparing procedures.
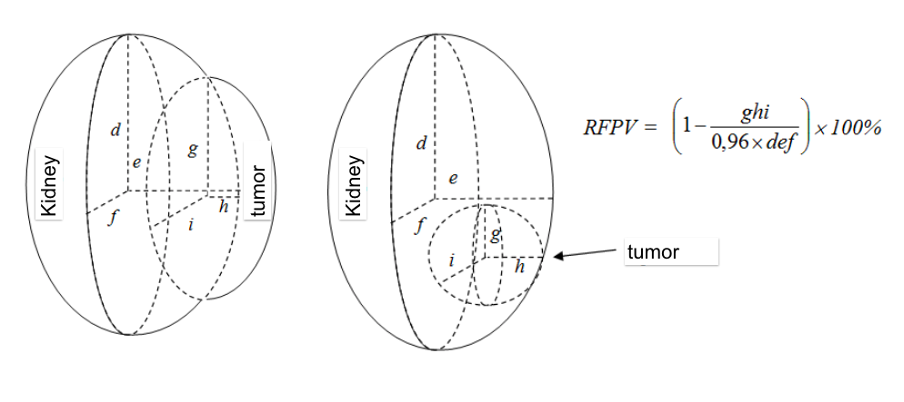
Visual depiction of the calculation of the remaining functioning parenchyma volume (RFPV)
In the pursuit of establishing unified standards, the aim of this study was to determine the key factors influencing the choice of surgical treatment for patients with localized RCC based on clinical and nephrometry data.
A retrospective study of 903 patients with localized RCC (T1-T2 N0 M0) who underwent surgical treatment from 2010 to 2017 was conducted. Patients were divided into two groups depending on the type of treatment: PN (n = 658) and RN (n = 245). The study groups did not differ statistically in terms of age, sex, ECOG status, body mass index (BMI), the number of patients with CKD, glomerular filtration rate (Mann-Whitney test; P = 0.08), hemoglobin levels (U-test, P = 0.08), and blood creatinine levels (U-test, P = 0.06).
The primary focus of this study was to determine tumor location, size, and to measure the remaining functional parenchymal volume as a key predictor of the percentage of the kidney that can be preserved during surgery. A subsequent multifactorial analysis was conducted on a large cohort of patients with available RFPV data. To determine the relationship between the risk of radical versus partial nephrectomy, a multifactorial predictive modeling method including 12 parameters was used. The main nephrometric parameters of tumor location in the kidney were analyzed according to the R.E.N.A.L. nephrometry score.
No statistically significant differences were found between the study groups regarding anatomical and topographic parameters such as tumor growth type, distance to the renal collecting system, tumor location, or its relationship to the interpolar line (P > 0.05). However, a significant difference was observed between the PN and RN groups in terms of tumor size, tumor location, and remaining functional parenchymal volume (P < 0.0001).
As a result of multifactorial analysis on a large cohort of RCC patients, it was determined that RFPV and tumor location are critical factors in determining the type of surgery. For polar and lateral tumor localization, the indication for partial nephrectomy was an RFPV greater than 58% and 67%, respectively. However, for medial tumors, the primary indication for PN was a tumor size of less than 38 mm. This study demonstrated that tumor size is relevant only for centrally located tumors.
Our findings confirm the value of a personalized approach to planning PN, where individual factors play a decisive role in surgical decision-making. Based on the study's findings, a specialized nephrometry system called NCIU (Nearness, Collateral, Inferior, Upper) was developed (picture 2). This system provides a comprehensive assessment of kidney tumors, indicating their location using letter-based classification and quantifying the tumor-free parenchyma volume for peripheral tumors, while considering lesion size for centrally located ones. The formula was integrated into an algorithm that evaluates the feasibility of partial nephrectomy for each individual case, allowing for a personalized surgical approach (for access to the online calculator, visit: https://calculator-kidney-cancer.com/).

Kidney separation into segments: N (nearness) for the central location; C (collateral), lateral lesions; and U (upper) and I (inferior), polar tumors.
We recommend integrating tumor location and RFPV indicators into nephrometry assessment to guide surgical strategies for RCC, tumors of a solitary kidney, recurrent renal tumors, kidney tumors in CKD, and other similar cases.
Overall, our study supports a comprehensive approach to kidney preservation, suggesting that the choice of surgical strategy depends on RFPV, tumor location, and tumor size. This will help standardize decision-making processes regarding nephron-sparing treatment strategies for RCC.
Written by: Professor Eduard Stakhovsky, Department of Plastic and Reconstructive Oncourology, National Cancer Institute of Ukraine, Kyiv, Ukraine.
References:
- Huang WC, Levey AS, Serio AM, Snyder M, Vickers AJ, Raj GV, et al. Chronic kidney disease after nephrectomy in patients with renal cortical tumours: a retrospective cohort study. Lancet Oncol 2006;7:735–40.
- Cirillo M, Lombardi C, Mele AA, Marcarelli F, Bilancio G. A population-based approach for the definition of chronic kidney disease: the CKD Prognosis Consortium. J Nephrol 2012;25:7–12.
- MacLennan S, Imamura M, Lapitan MC, Omar MI, Lam TB, Hilvano-Cabungcal AM, et al. UCAN Systematic Review Reference Group; EAU Renal Cancer Guideline Panel. Systematic review of perioperative and quality-of-life outcomes following surgical management of localised renal cancer. Eur Urol 2012;62:1097–117.
- Motzer RJ, Jonasch E, Michaelson MD, et al. NCCN Guidelines Insights: Kidney Cancer, Version 2. 2020. J Natl Compr Canc Netw 2019;17(11):1278–85.
- Ljungberg B, AlbigesL, Abu-Ghanem Y, et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2019 Update. Eur Urol 2019; 75(5): 799–810.
- MacLennan S, Imamura M, Lapitan MC, Omar MI, Lam TB, Hilvano-Cabungcal AM, et al. UCAN Systematic Review Reference Group, EAU Renal Cancer Guideline Panel. Systematic review of oncological outcomes following surgical management of localised renal cancer. Eur Urol 2012;61:972–93; erratum: Eur Urol 2012;62:193.
- Kutikov A, Uzzo RG. The R.E.N.A.L. nephrometry score: a comprehensive standardized system for quantitating renal tumor size, location and depth. J Urol. 2009 Sep;182(3):844-53. doi: 10.1016/j.juro.2009.05.035. Epub 2009 Jul 17. PMID: 19616235.
- Ficarra V, Porpiglia F, Crestani A, Minervini A, Antonelli A, Longo N, Novara G, Giannarini G, Fiori C, Simeone C, Carini M, Mirone V. The Simplified PADUA REnal (SPARE) nephrometry system: a novel classification of parenchymal renal tumours suitable for partial nephrectomy. BJU Int. 2019 Oct;124(4):621-628. doi: 10.1111/bju.14772. Epub 2019 May 7. PMID: 30963680.
- Gupta R, Tori M, Babitz SK, Tobert CM, Anema JG, Noyes SL, Lane BR. Comparison of RENAL, PADUA, CSA, and PAVP Nephrometry Scores in Predicting Functional Outcomes After Partial Nephrectomy. Urology. 2019 Feb;124:160-167. doi: 10.1016/j.urology.2018.03.055. Epub 2018 Aug 11. PMID: 30107186.
- Weprin S, Falagario U, Veccia A, Nandanan N, Emerson D, Ovanez C, Albuquerque EV, Zukovski EB, Clayton R, Hampton L, Autorino R. Simplified PADUA Renal (SPARE) Nephrometry Scoring System: External Validation, Interobserver Variability, and Comparison with RENAL and PADUA in a Single-center Robotic Partial Nephrectomy Series. Eur Urol Focus. 2021 May;7(3):591-597. doi: 10.1016/j.euf.2020.05.016. Epub 2020 Jun 23. PMID: 32591285.
- Schindl MJ, Redhead DN, Fearon KC, Garden OJ, Wigmore SJ; Edinburgh Liver Surgery and Transplantation Experimental Research Group (eLISTER). The value of residual liver volume as a predictor of hepatic dysfunction and infection after major liver resection. Gut. 2005 Feb;54(2):289-96. doi: 10.1136/gut.2004.046524. PMID: 15647196; PMCID: PMC1774834.