The clinical role of post-RLT biodistribution imaging has been assessed in prostate cancer (PCa), showing that [177Lu]Lu-PSMA-617 SPECT/CT can impact patient management in up to 49% of cases at almost zero cost,3 and provide prognostic volumetric parameters.4 However, only a few papers evaluated the predictive role of SPECT. In our paper,5 we aimed to determine whether semiquantitative biodistribution parameters obtained from the 1st cycle [177Lu]Lu-PSMA-617 SPECT/CT can predict response to RLT at the lesion level. Specifically, we considered a total of 23 advanced mCRPC patients who received at least two [¹⁷⁷Lu]Lu-PSMA-617 cycles at Messina and Genova Universities, performing a complete SPECT/CT at the 1st RLT cycle. Each [¹⁷⁷Lu]Lu-PSMA-617-positive lesion, well differentiated from the background, was semiautomatically segmented through a 40% threshold to extract SUVmax, SUVmean, Total Lesion Volume (TLV), and the Total Lesion Activity (TLA=SUVmean×TLV). Each lesion parameter was then correlated with the single-lesion response at the last RLT cycle, classified as progressive (PD) or non-PD (complete/partial response, or stable disease) according to a composite gold standard based on suggested cut-off from qualitative RECIP 1.0 and quantitative PPP criteria.6,7
Namely, the single lesion was considered as PD at the last RLT cycle in case of PSMA-volume increase ≥20% or PSMA-uptake increase ≥30% at [¹⁷⁷Lu]Lu-PSMA-617 SPECT/CT (end of treatment PSMA and/or FDG PET were eventually used for doubtful cases). We obtained a total of 290 lesions (249 were osteomedullary, 34 lymph nodal, and 7 visceral), of which 60 were classified as PD at the last RLT (56/60 osteomedullary, 3/60 lymph nodal, 1/60 visceral from the liver). The two-tailed Mann-Whitney U test showed that SUVmax, SUVmean, TLV, and TLA from baseline [¹⁷⁷Lu]Lu-PSMA-617 SPECT/CT were significantly higher in non-PD than in PD lesions (p<0.05). Baseline TLA, SUVmax, SUVmean, and TLV optimal cut-offs for predicting the single-lesion response at the last RLT cycle using the area under the ROC curve (AUC), were as follows: TLA AUC 0.854 (best cut-off 61.7, sens 66.5%, spec 88.3%), SUVmax AUC 0.843 (best cut-off 11.8, sens 67.4%, spec 91.7%), SUVmean AUC 0.838 (best cut-off 6, sens 73.9%, spec 85%), TLV AUC 0.612 (best cut-off 7.05mL, sens 65.2%, spec 56.7%). In Figure 1, we reported exemplary responding and progressive lesions from the same patient.
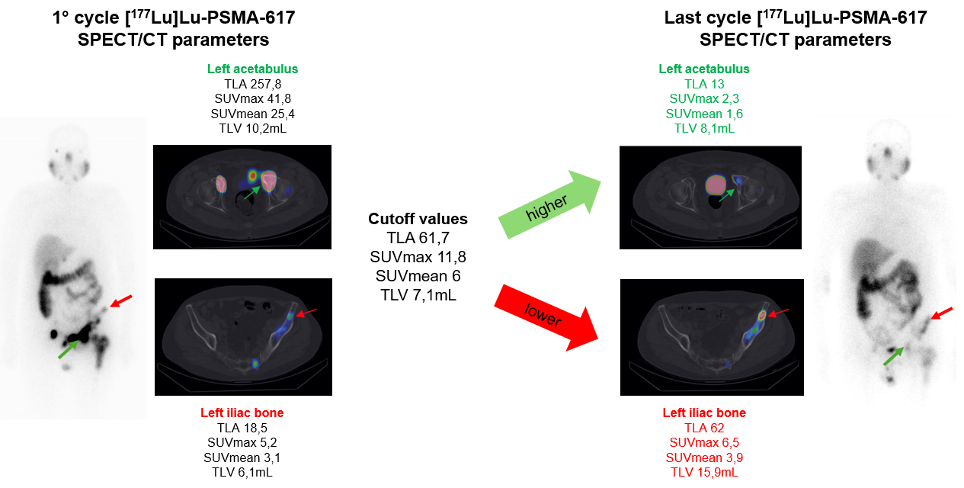
Despite limitations (small cohort, the retrospective nature, the missing of an external validation, the potential suboptimal gold standard), our preliminary study further shed light on the value of biodistribution SPECT/CT that uses exactly the same RLT radionuclide, can be performed after each cycle at almost zero cost (except scanner usage time), reducing the need of PSMA PET, lowering radiation exposure, and enhancing prognostic consideration. All analyzed PSMA-based baseline SPECT parameters were statistically higher in non-progressive than in progressive lesions, indicating a potential association between receptor expression intensity at biodistribution SPECT/CT and therapeutic response. This is already known for PSMA PET, where higher PSMA expression, as measured by SUVmean, can predict a favourable response to [177Lu]Lu-PSMA-617 RLT.8,9
Less intuitive can be the result relating to TLA, which is nevertheless an expression of the product between SUVmean and lesion/disease volume, which could imply a favourable response to treatment for those lesions with high PSMA expression, even if with high volume (TLV). In conclusion, we have preliminarily shown that [177Lu]Lu-PSMA-617 SPECT/CT semiquantitative parameters can predict the single-lesion response to RLT, early highlighting potential non-responding lesions (1st cycle TLA<61.7, SUVmax<11.8, SUVmean<6, TLV<7.05mL) to be closely monitored, considering additional/focused therapy.
Written by: Riccardo Laudicella,1 Greta Celesti,1 Matteo Bauckneht,2,3 Agatino Micali,4 Federica Midili,4 Antonio Bucca,5 Victorian M Ferro,5 Michela Piergentili,2 Giorgia Ricciardello,1 Anna Brogna,4 Benedetta Pagano,1 Sergio Baldari,1 Irene A Burger,6,7 Fabio Minutoli1
- Nuclear Medicine Unit, Department of Biomedical and Dental Sciences and Morphofunctional Imaging, University of Messina, Messina, Italy.
- IRCCS Azienda Ospedaliera Metropolitana, Genova, Italy.
- Department of Health Sciences (DISSAL), University of Genova, Genova, Italy.
- Health Physics Unit, Messina University Hospital G. Martino, Messina, Italy.
- Health Physics School of Specialization, Department of Biomedical and Dental Sciences and Morphofunctional Imaging, University of Messina, Messina, Italy.
- Department of Nuclear Medicine, Faculty of Medicine, Kantonsspital Baden, affiliated Hospital for Research and Teaching, University of Zurich, Baden, Switzerland.
- Department of Nuclear Medicine, University Hospital Zurich, University of Zurich, Zurich, Switzerland.
- Kratochwil C et al. Joint EANM/SNMMI procedure guideline for the use of 177Lu-labeled PSMA-targeted radioligand-therapy (177Lu-PSMA-RLT). Eur J Nucl Med Mol Imaging. 2023;50:2830-2845.
- Uribe C et al. Summary: SNMMI/ACNM Procedure Standard for Posttreatment Imaging of 177Lu-Based Radiopharmaceuticals. J Nucl Med. 2025;66:1528-1537.
- Yadav S et al. Impact of Posttreatment SPECT/CT on Patient Management During 177Lu-PSMA-617 Radiopharmaceutical Therapy. J Nucl Med. 2024;65:1395-1401.
- Alkahtani TO. Investigating the significance of SPECT/CT-SUV for monitoring 177Lu-PSMA-targeted radionuclide therapy: a systematic review. BMC Med Imaging. 2025;25:28.
- Laudicella R et al. The predictive role of [177Lu]Lu-PSMA-617 SPECT/CT semiquantitative parameters from the 1st RLT cycle in advanced mCRPC: a preliminary bicentric lesion-based analysis. Eur J Nucl Med Mol Imaging. 2026 May 20.
- Unterrainer LM et al. Evidence-Based Clinical Protocols to Monitor Efficacy of [177Lu]Lu-PSMA Radiopharmaceutical Therapy in Metastatic Castration-Resistant Prostate Cancer Using Real-World Data. J Nucl Med. 2025;66:1054-1060.
- Fanti S et al. Proposal for Systemic-Therapy Response-Assessment Criteria at the Time of PSMA PET/CT Imaging: The PSMA PET Progression Criteria. J Nucl Med. 2020;61:678-682.
- Buteau JP et al. PSMA and FDG-PET as predictive and prognostic biomarkers in patients given [177Lu]Lu-PSMA-617 versus cabazitaxel for metastatic castration-resistant prostate cancer (TheraP): a biomarker analysis from a randomised, open-label, phase 2 trial. Lancet Oncol. 2022;23:1389-1397.
- Kuo PH et al. Quantitative 68Ga-PSMA-11 PET and Clinical Outcomes in Metastatic Castration-resistant Prostate Cancer Following 177Lu-PSMA-617 (VISION Trial). Radiology. 2024;312:e233460.