These multimodal therapy strategies improve outcomes on average, but also impose a considerable cumulative burden on the patient, e.g., metabolic and sexual consequences of sustained castration, fatigue, cardiovascular risk, and financial toxicity. The field has lacked a prospectively validated method for matching treatment intensity to underlying disease biology at the individual patient level. ProBio-mHSPC was designed around the premise that “more” should not be the default for every patient, and “less” should not be offered blindly.
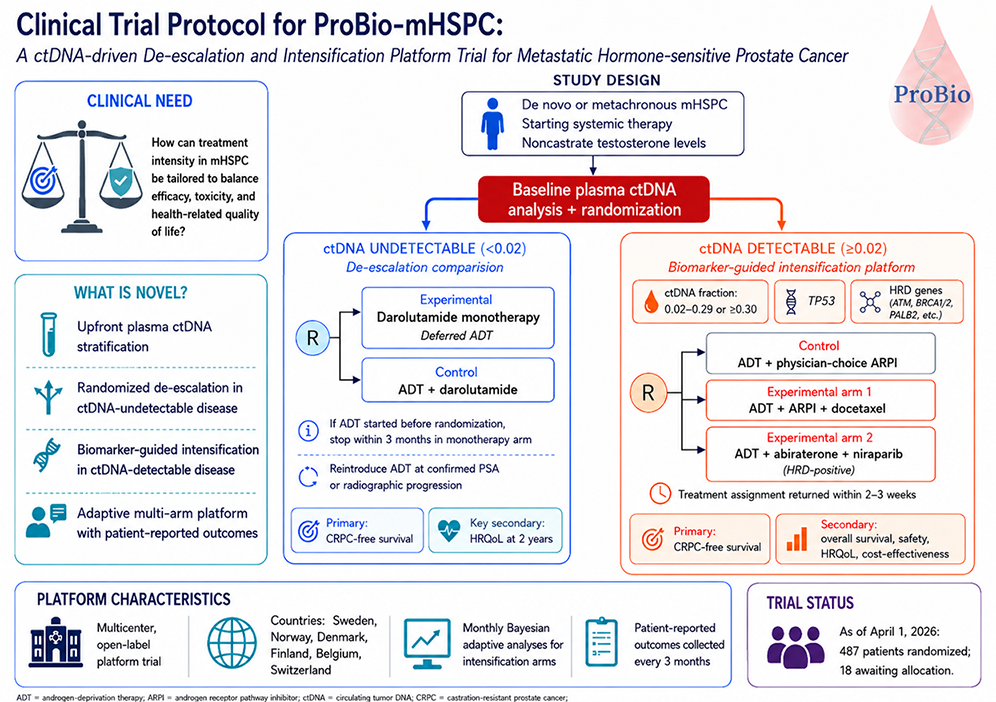
The novelty of ProBio is its use of circulating tumor DNA (ctDNA) as an upfront decision tool, rather than as a retrospective prognostic marker or exploratory assay. A baseline liquid biopsy guides patients into two clinically distinct populations, each entering a separate randomized framework. Patients with undetectable ctDNA, reflecting a systemic tumor burden below the analytical threshold of the assay, are allocated to a noninferiority de-escalation comparison of darolutamide monotherapy with deferred ADT against continuous ADT plus darolutamide. Patients with detectable ctDNA enter a biomarker-guided intensification platform in which ctDNA fraction, TP53 mutational status, and homologous recombination deficiency (HRD) direct allocation to intensified systemic strategies, including docetaxel-containing triplets or niraparib combined with abiraterone acetate for HRD-positive disease. ProBio’s biomarker framework underpins both questions simultaneously, i.e., identifying patients for whom treatment burden might safely be reduced and those for whom it should be escalated.
Testing de-escalation strategies in mHSPC has to date been predominantly response-adaptive, typically employing PSA-guided modification or interruption of ADT following an induction period of ADT plus an ARPI. ProBio takes a different route. It asks whether the absence of detectable ctDNA at baseline can identify a population with a sufficiently favorable tumor biology to support early ADT deferral. The trial does not merely pause therapy after a response; it challenges the necessity of immediate continuous castration in a molecularly selected subgroup. This is a bold but patient-centered hypothesis, supported by safeguards: a noninferiority design, prospective collection of patient-reported outcomes, independent Data Safety Monitoring Board oversight, and predefined PSA-based criteria for ADT reintroduction.
Equally novel is the intensification strategy. Detectable ctDNA is not deployed as a simple binary indicator of poor prognosis. Instead, ProBio uses the liquid biopsy to define biologically informed subgroups and adapts randomization probabilities as trial evidence accumulates. This is particularly relevant in a disease landscape where the standard of care evolves rapidly, and conventional trial designs can be rendered obsolete before primary endpoint readout. The platform structure, concurrent controls, and predefined decision rules for graduation or futility allow efficient evaluation of multiple therapy-biomarker combinations within a single infrastructure.
For the practicing uro-oncologist, the broader implication of ProBio is that a liquid biopsy may become a practical, first-line clinical decision tool for assigning treatment intensity, not merely for molecular annotation. It embeds patient-reported outcomes and cost-effectiveness assessment alongside survival endpoints, acknowledging that therapeutic value must be measured across multiple dimensions.
If successful, ProBio could move mHSPC care beyond clinicopathologic risk groups and imaging-defined disease volume toward dynamic, minimally invasive precision medicine, where treatment intensity is matched to tumor biology and to what matters most to patients.
Written by: Bram De Laere,1 Alessio Crippa,2 Andrea Discacciati,2 Ashkan Mortezavi,3 Christoph Müller,4 Andreas Røder,5 Antti Rannikko,6 Piet Ost,7 Martin Eklund,2 Johan Lindberg,2 Henrik Grönberg,8 ProBio Investigators
- Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden; Department of Human Structure and Repair Ghent University, Ghent, Belgium.
- Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden.
- Universitätsspital Zürich, Zürich, Switzerland.
- Cancer Treatment Centre, Sorlandet Hospital, Kristiansand, Norway.
- Urological Research Unit, Department of Urology, Center for Cancer and Organ Diseases Copenhagen University Hospital - Rigshospitalet, Denmark; Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark.
- Research Program in Systems Oncology, Research Programs Unit and iCAN-Digital Precision Cancer Medicine Flagship, Faculty of Medicine, University of Helsinki, Helsinki, Finland; Department of Urology, Helsinki University Hospital, Helsinki, Finland.
- Department of Human Structure and Repair Ghent University, Ghent, Belgium; Department of Radiation Oncology, Iridium Network, Wilrijk, Belgium.
- Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden.
Read the Abstract