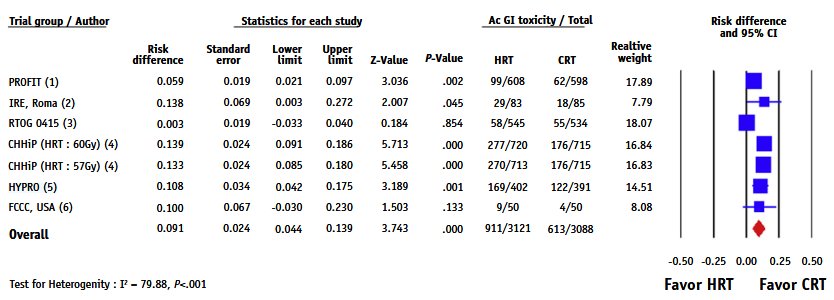
However, across the literature,2 moderate hypofractionated radiotherapy is associated with increased acute grade 2 gastrointestinal (GI) toxicity:2
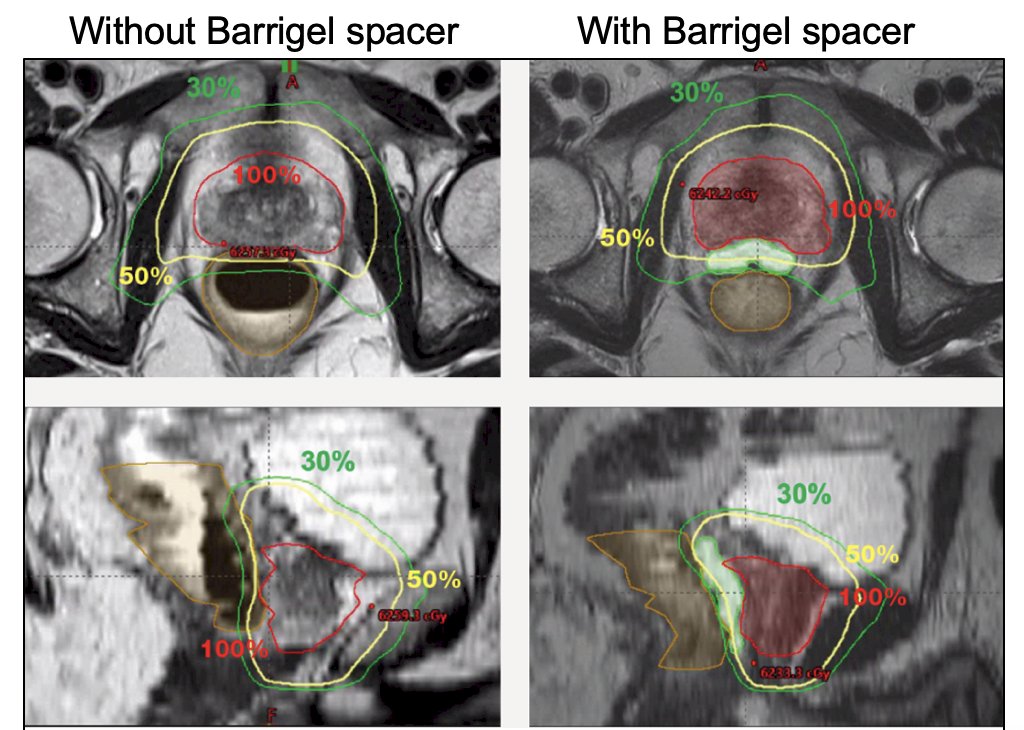
In 2023, Mariados et al.3 reported the primary analysis of a trial assessing the safety and efficacy of stabilized hyaluronic acid as a rectal spacer. From March 2020 to June 2021, patients with low or intermediate risk prostate cancer undergoing moderate hypofractionated radiotherapy (60 Gy in 20 fx) were randomized (2:1) to Barrigel rectal spacer + fiducial markers (n = 136) versus a fiducial marker control arm (n = 65):
Patients were stratified by: (i) ADT (0 versus 4 months), (ii) erectile function (good versus poor EPIC-26), and (iii) geographic region. The dosimetry metrics for the trial were as follows:
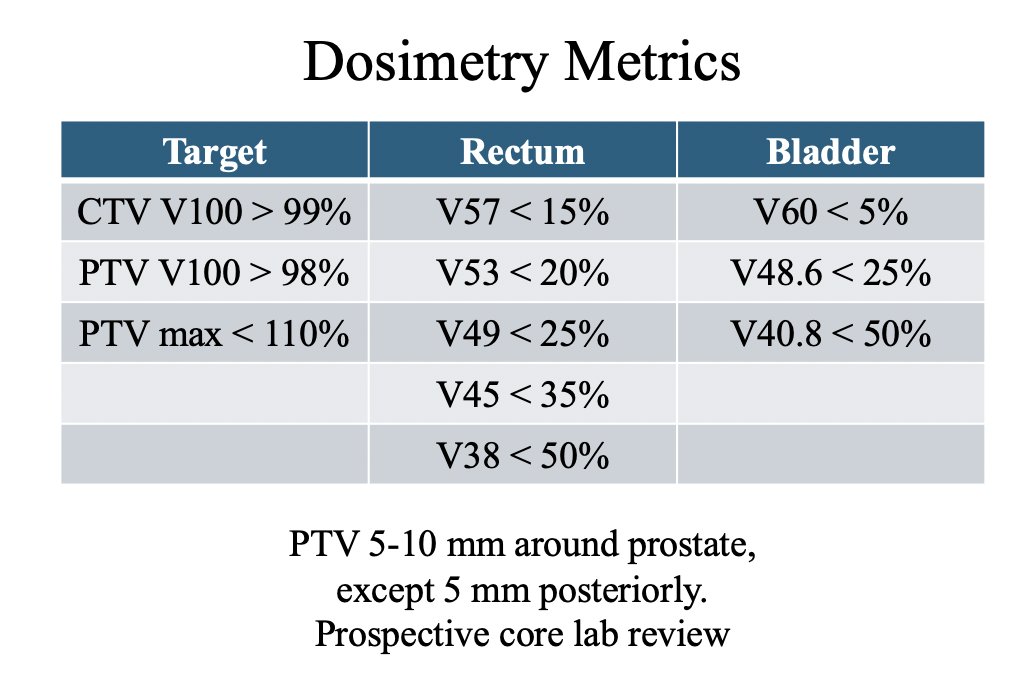
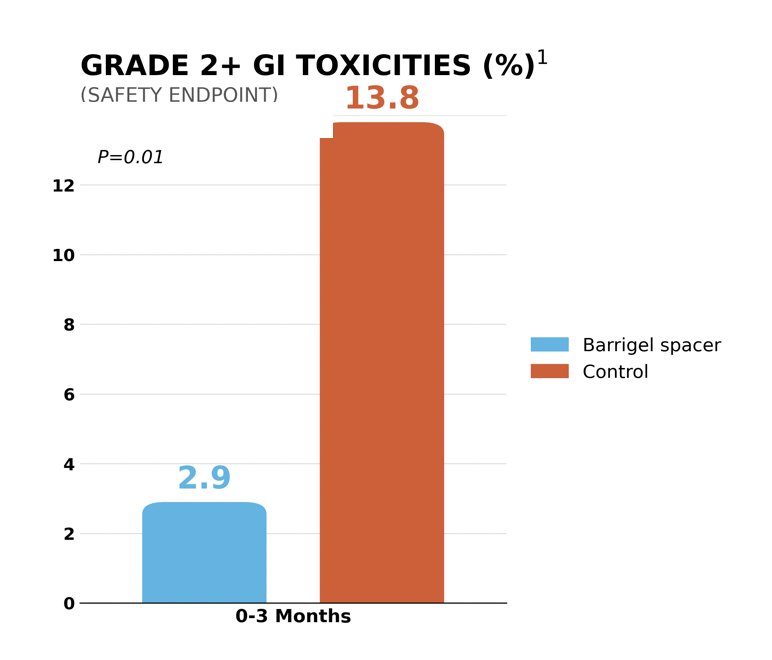
The primary endpoint was met: 98.5% of patients receiving a Barrigel rectal spacer achieved a >25% reduction in rectal V54 Gy (V90%). Additionally, the key secondary endpoint was patient safety: rectal spacing reduced acute (0-3 months) grade 2+ GI toxicity (2.9%) compared to the control arm (13.8%; p = 0.01):
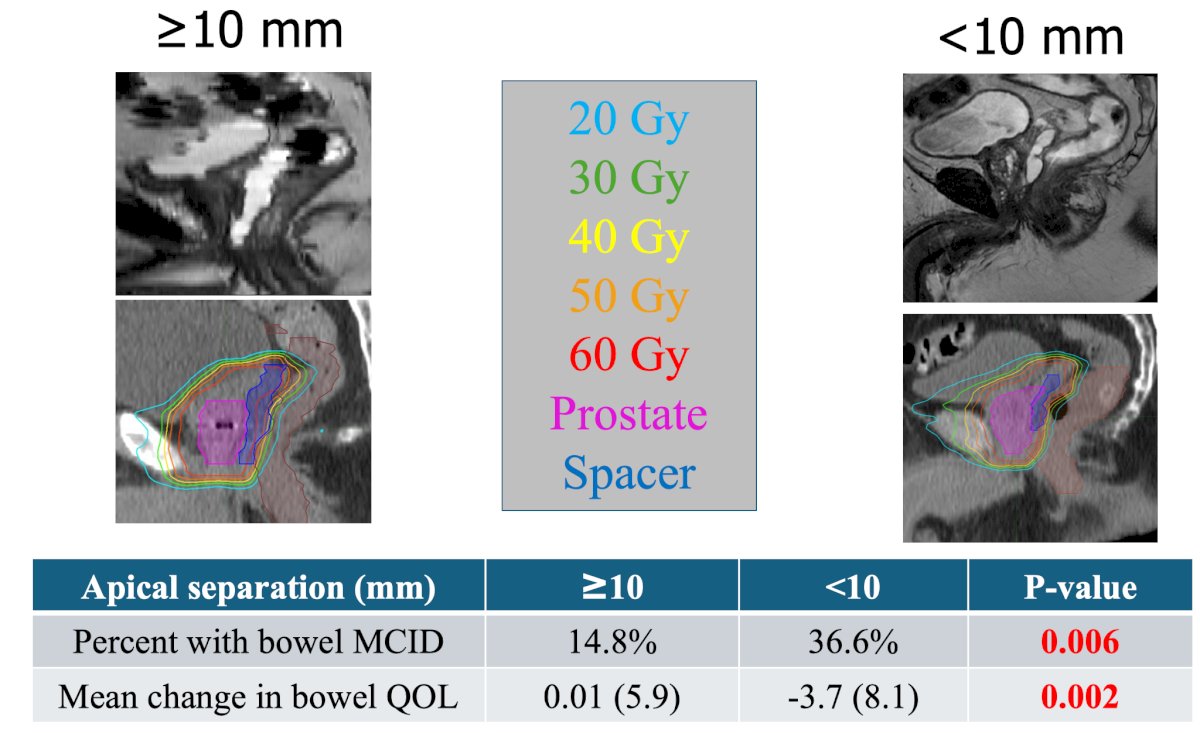
In a secondary analysis of the pivotal trial, King et al.4 reported that greater apical spacing (> 10 mm) was associated with improved rectal dosimetry and a smaller decline in bowel quality of life at 3 months:
The objectives of this subsequent analysis of the Barrigel pivotal trial were to evaluate whether hyaluronic acid spacers reduce late (6-36 months) (i) grade 2+ GI events, and (ii) grade 2+ genitourinary (GU) events. The cumulative incidences of late (6-36 months from baseline) grade 2+ GI and GU toxicities were assessed via CTCAE v5.0 and compared with the log-rank test. The percentages of patients with differences in bowel MCID (5 points) at 36 months across treatment groups were compared with a 2-sided Pearson Chi-squared test, as well as testing an association with adequate apical spacing.
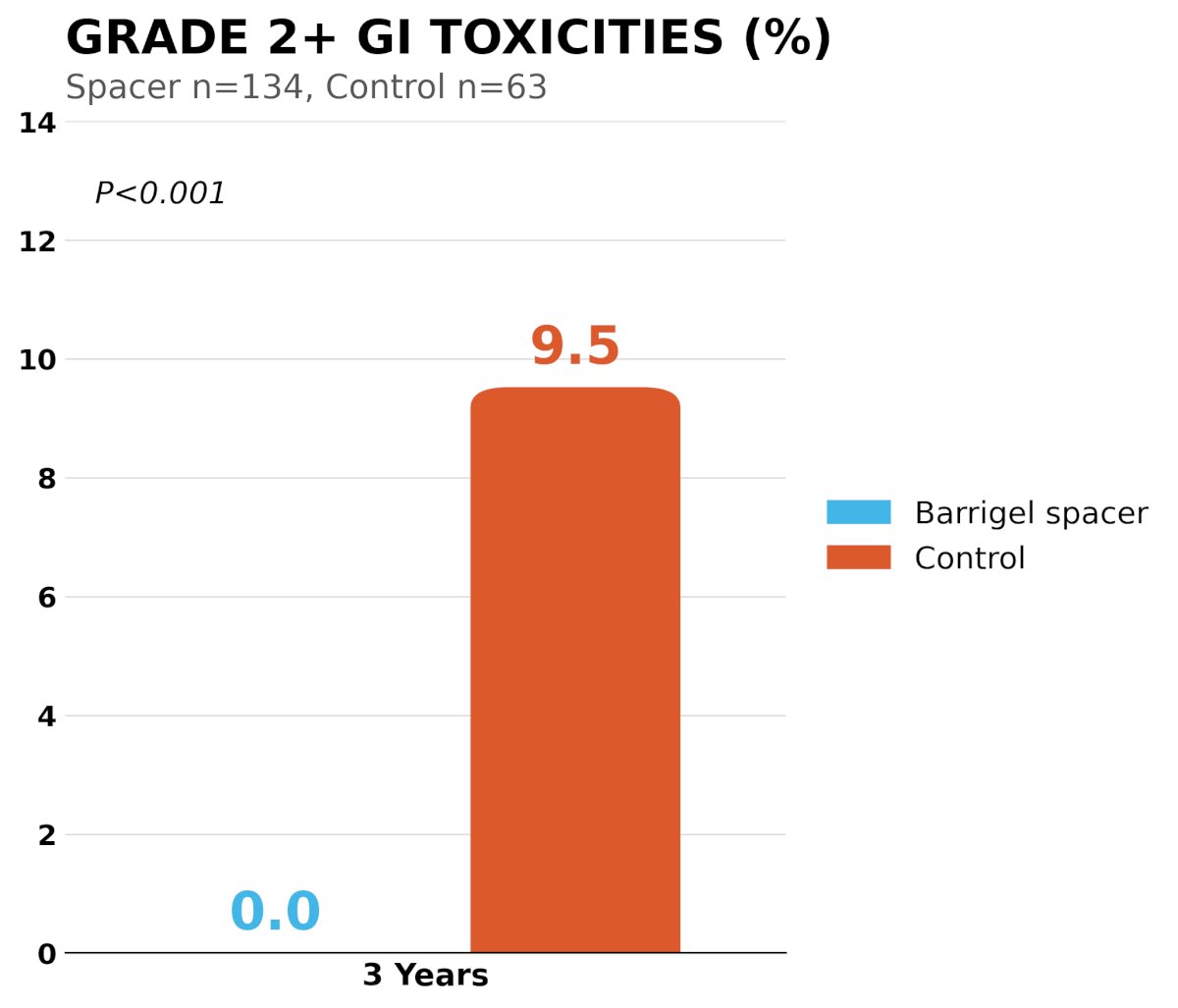
For this subsequent late toxicity analysis, grade 2+ GI toxicity at 3 years was significantly decreased (p < 0.001) between the Barrigel rectal spacer arm (0%) and the control arm (9.5%):
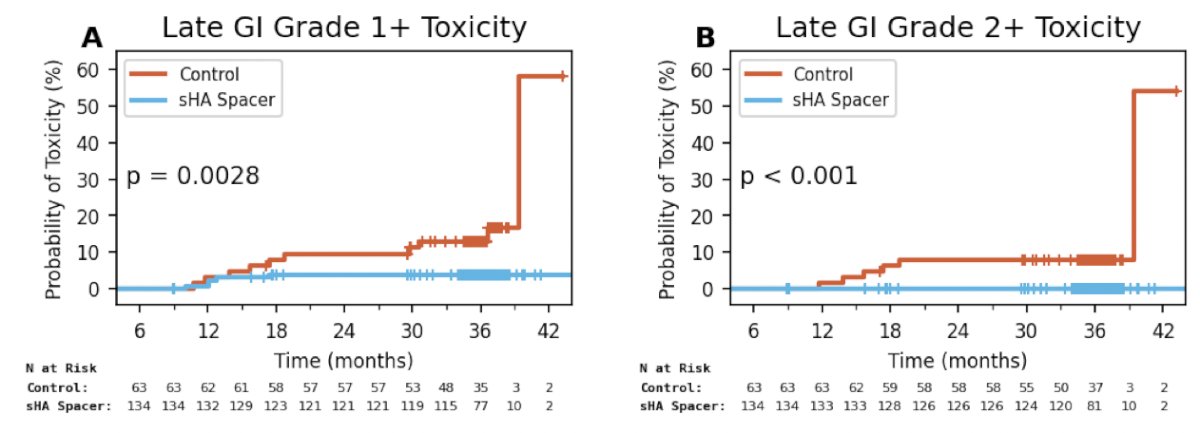
In an assessment of the probability of toxicity over time, there was significantly higher risk of late GI grade 1+ (p = 0.0028) and grade 2+ (p < 0.001) toxicity for the control arm versus the Barrigel rectal spacer arm:
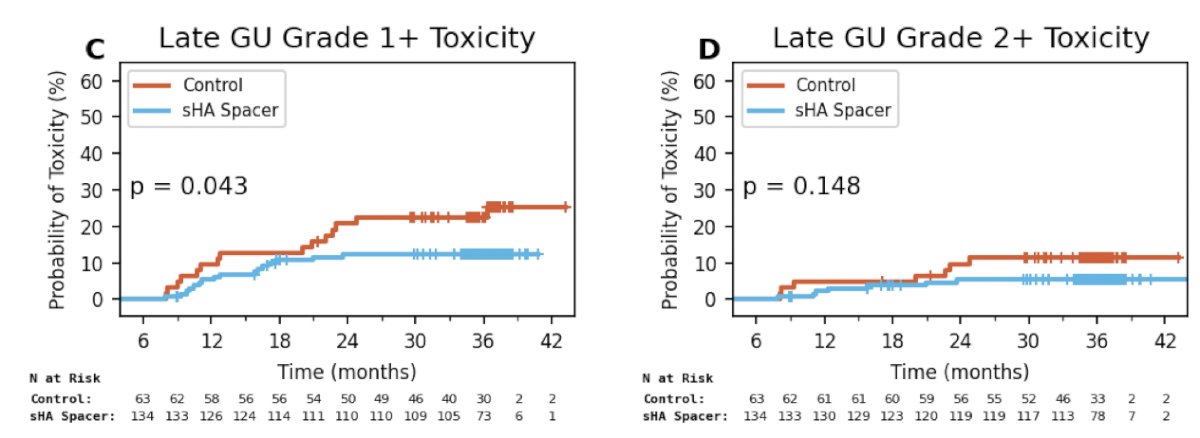
In a similar assessment of late GU grade 1+ and grade 2+ toxicity, there was a significantly higher risk of toxicity over time for the control group for grade 1+ toxicity (p = 0.043), but not for grade 2+ (p = 0.148) toxicity:
When assessing the dose volume histogram (DVH), the optimal dosimetry5 was 99% for Barrigel rectal spacer versus 96% for the control group:
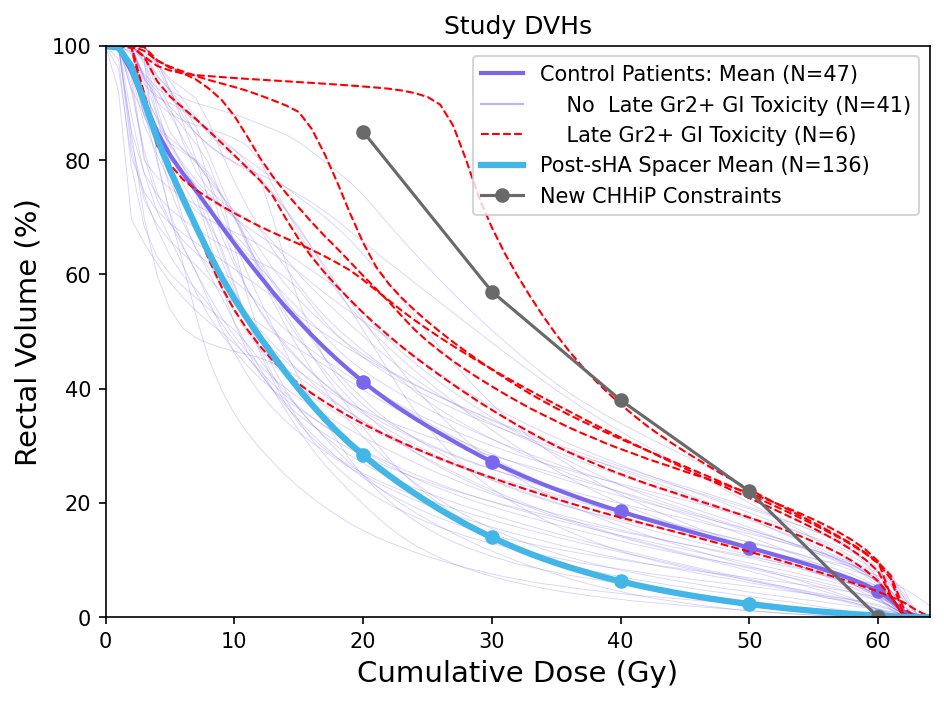
Of note, 5 of 6 patients with late grade 2+ GI toxicity in the control arm had worse rectal dosimetry.
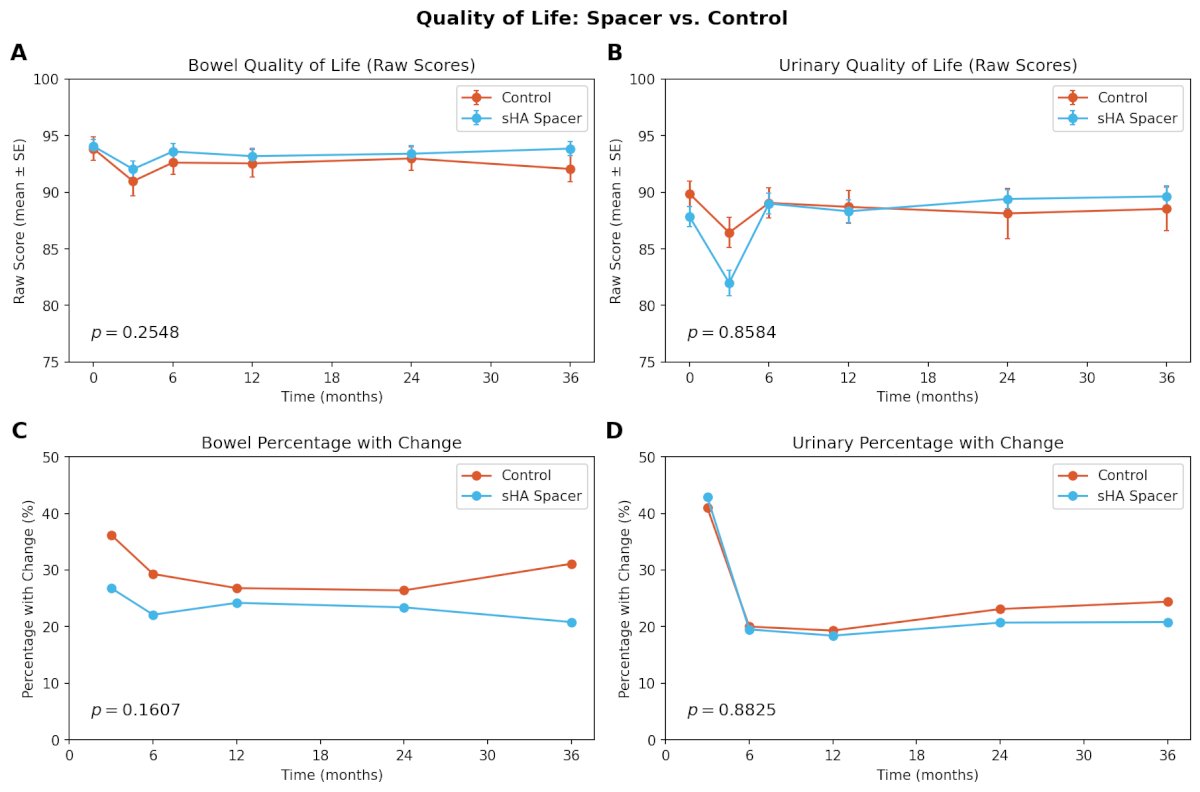
For the quality of life assessment, 151 (76.1%) patients had submitted EPIC questionnaires at 36 months. There was no difference in bowel or urinary quality of life across treatment arms at 36 months:
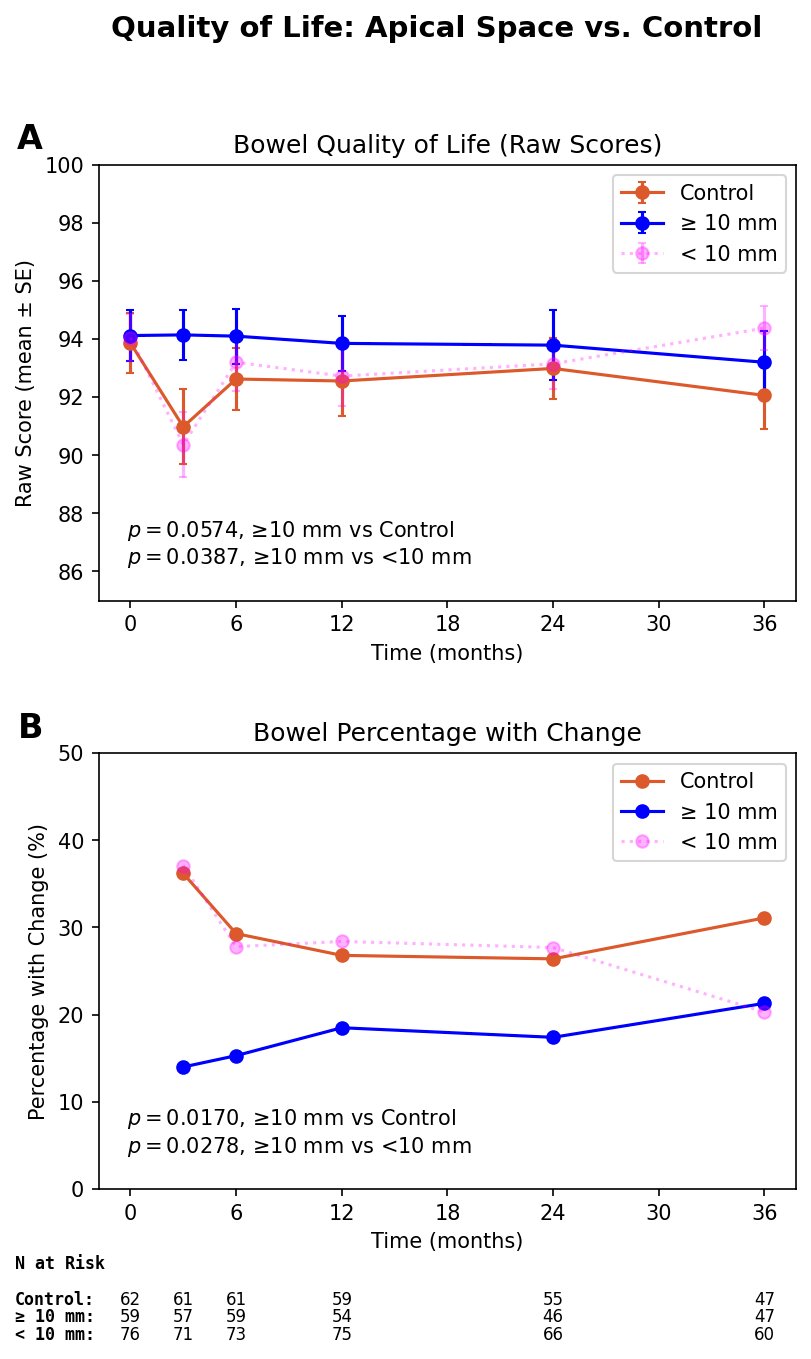
In the apical spacing analysis, the Barrigel rectal spacer group was divided into patients with >=10 mm versus <10 mm of apical space. Patients with >=10 mm of apical space had improved bowel quality of life at 3 years:
Dr. King concluded his presentation discussing 3-year results from a prospective multicenter randomized controlled trial of stabilized hyaluronic acid spacer for hypofractionated prostate radiation therapy with the following take home points:
- Stabilized hyaluronic acid rectal spacer was associated with a durable reduction in late grade 2+ GI toxicities, despite excellent contemporary rectal dosimetry in the control arm
- Rectal spacing may provide the greatest patient reported benefit when the implant geometry achieves adequate (>1 cm) of apical separation
Presented by: Martin King, MD, PhD, Dana-Farber and Brigham and Women’s Cancer Center, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on X during the European Society of Radiotherapy and Oncology (ESTRO) 2026 Annual Meeting, Stockholm, Sweden, Fri, May 15 – Tues, May 19, 2026.
References:
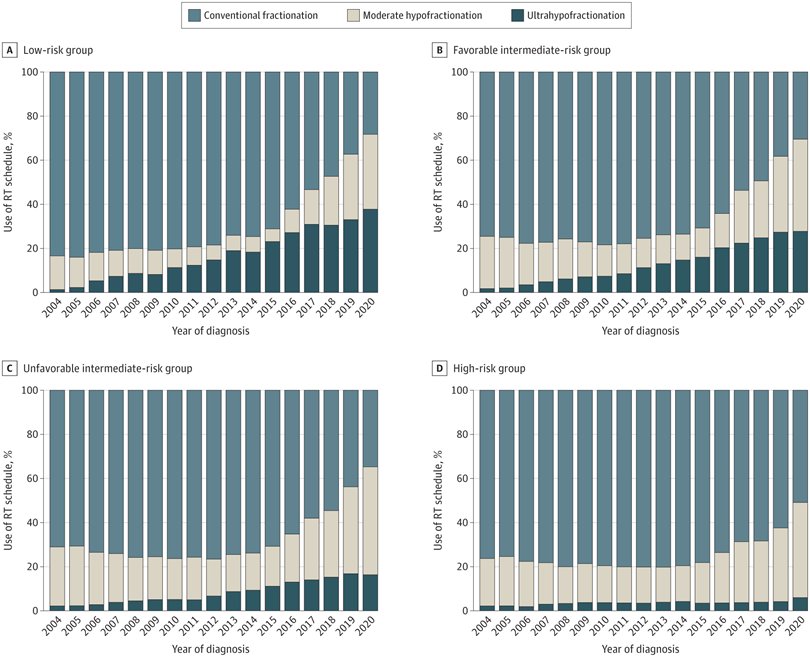
- Yu JB, Sun Y, Jia AJ, et al. Increasing use of shorter-course radiotherapy for prostate cancer. JAMA Oncol. 2023 Dec 1;9(12):1696-1701.
- Datta NR, Stutz E, Rogers S, et al. Conventional versus hypofractionated radiation therapy for localized or locally advanced prostate cancer: A systematic review and meta-analysis along with therapeutic implications. Int J Radiat Oncol Biol Phys. 2017 Nov 1;99(3):573-589.
- Mariados NF, Orio 3rd PF, Schiffman Z, et al. Hyaluronic acid spacer for hypofractionated prostate radiation therapy: A randomized clinical trial. JAMA Oncol. 2023 Apr 1;9(4):511-518.
- King MT, Svator M, Chell EW, e tla. Evaluating the quality-of-life effect of apical spacing with hyaluronic acid prior to hypofractionated prostate radiation therapy: A secondary analysis. Pract Radiat Oncol. 2024 May-Jun;14(3):e214-e219.
- Wilkins A, Naismith O, Brand D, et al. Derivation of dose/volume constraints for the anorectum from clinician- and patient-reported outcomes in the CHHiP trial of radiation therapy fractionation. Int J Radiat Oncol Biol Phys. 2020 Apr 1;206(5):928-938.