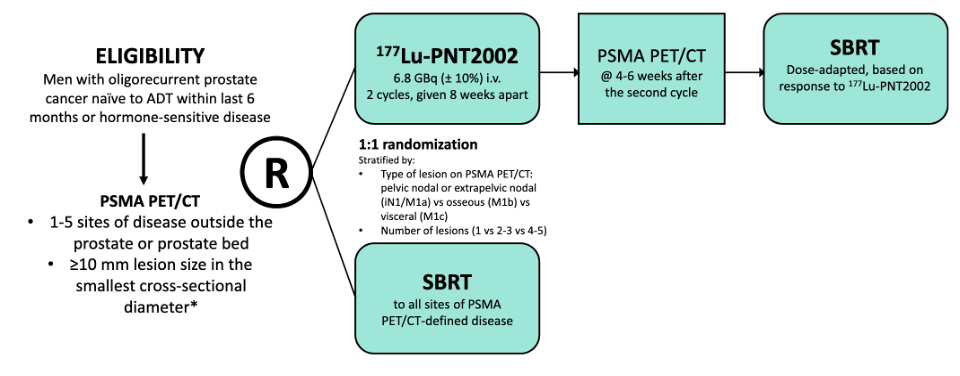
Figure 1: Simplified Study Design
In total, 100 patients were assessed for eligibility, and 92 were enrolled in the study. 45 patients received the interventional therapy consisting of 2 cycles of 177Lu-PSMA-I&T followed by SBRT. During the first cycle of therapy, multiple timepoint SPECT/CT imaging was acquired, allowing for evaluation of absorbed dose estimates (Figure 2).

Figure 2: Patients randomized to the intervention arm timetable of therapy and imaging
As patients are treated at earlier disease stages with radiopharmaceutical therapies, adverse events are a potential concern; the most common events associated with 177Lu-PSMA radiopharmaceutical therapies based on the VISION Trial included fatigue, mild xerostomia, and nausea. Other concerns included nephrotoxicity and bone marrow toxicity.
Herein, the goal of this manuscript was to evaluate the absorbed doses to lesions and organs at risk. An example of oligometastatic hormone-sensitive prostate cancer patients included in the interventional arm of the study is found in Figure 3.
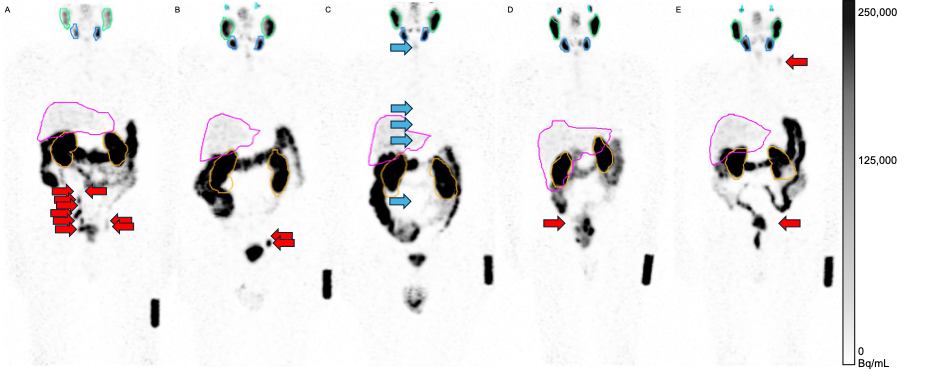
Figure 3: Representative SPECT maximum intensity projections (anterior to posterior) at 24 hours post-injection 177Lu-PSMA-I&T. All lesions shown in red are LN-based, and blue (only patient (C)) are bone-based. (A) patient with the most individual lesions treated (n = 9). (B) The lesion with the greatest tumor-to-background ratio was included. (C) Greatest overall tumor volume (GTV-based: 36.0 mL, PTV-based: 145.9 mL). (D) Lowest overall tumor volume (GTV-based: 0.5 mL, PTV-based: 1.9 mL). (E) Distant disease.
First, the lesions were often very small, leading to absorbed dose underestimates during dosimetric evaluation (even with a phantom-based recovery coefficient applied). Methods to address the limited spatial resolution of SPECT are required for accurate dosimetry in these small lesions (e.g., advanced reconstructions, deconvolution-based methods, AI, etc.). Regardless, we found that the addition of 177Lu-PSMA-I&T was mainly for microscopic disease, while SBRT was able to treat the visible lesions. This ultimately led to significantly improved PSMA PET/CT–based progression-free survival compared to patients treated without 177Lu-PSMA-I&T (median, 17.6 vs. 7.4 mo; hazard ratio, 0.37).
For normal organs, the estimated absorbed doses were within the range of prior reports (Table 1). omHSPC patients have low volume disease (total tumor volume of interventional arm LUNAR patients: 20.7 ± 25.3 mL), theoretically suggesting organs may receive a greater absorbed dose than typically published. This was not the case as organs remained within tolerable limits, and derived absorbed doses were comparable to published studies, indicating a lack of the tumor sink effect.
Table 1: All numerical values are shown in units of Gy/GBq. The last three rows represent tumor lesion AD [median], and n represents the number of lesions that were evaluated.

Written by: Zachary Ells,1 Catherine Meyer,1 Koichiro Kimura,1 Holly Wilhalme,2 Minsong Cao,3 Vinicius B. Ludwig,1 Lena M. Unterrainer,1,4 David Sennung,1 Rejah Nabong,1 Carol Felix,3 Luca F. Valle,3 Anthony Daley,1 Johannes Czernin,1 Magnus Dahlbom,1 Amar U. Kishan,3 Jeremie Calais1
- Department of Nuclear Medicine and Theranostics, Ahmanson Translational Theranostics Division, David Geffen School of Medicine, UCLA, Los Angeles, California.
- Department of Medicine Statistical Core, UCLA, Los Angeles, California.
- Department of Radiation Oncology, UCLA, Los Angeles, California.
- Department of Nuclear Medicine, TUM Klinikum, Rechts der Isar, Technical University of Munich, School of Medicine and Health, Munich, Germany.
** All values from the currently mHSPC studies have been from [177Lu]Lu-PSMA-617 through a series of publications from the same group.
References:
- Uijen MJM, Privé BM, van Herpen CML, et al. Kidney absorbed radiation doses for [177Lu]Lu-PSMA-617 and [177Lu]Lu-PSMA-I&T determined by 3D clinical dosimetry. Nucl Med Commun. 2023;44:270.
- Peters SMB, Privé BM, de Bakker M, et al. Intra-therapeutic dosimetry of [177Lu]Lu-PSMA-617 in low-volume hormone-sensitive metastatic prostate cancer patients and correlation with treatment outcome. Eur J Nucl Med Mol Imaging. 2022;49:460-469.
- Grob D, Privé BM, Muselaers CHJ, et al. Bone marrow dosimetry in low-volume mHSPC patients receiving Lu-177-PSMA therapy using SPECT/CT. EJNMMI Phys. 2024;11:34.