The continued use of systematic sampling alongside targeted biopsy has traditionally been justified by concerns that clinically significant tumours may exist outside MRI-visible lesions. While this strategy aims to maximise cancer detection, it comes at the cost of increased biopsy burden, including a higher number of cores, longer procedural times, greater patient discomfort, and a potential increase in complications. As diagnostic pathways evolve, refining biopsy strategies to preserve oncologic accuracy while minimising unnecessary sampling has become a key priority in contemporary prostate cancer diagnostics.
The TARGET clinical trial was designed to address this challenge by evaluating whether a more focused biopsy strategy could replace the traditional combination of targeted and systematic biopsies. Specifically, the study investigates the diagnostic performance of targeted biopsy combined with perilesional sampling, compared with the current standard approach of targeted plus systematic biopsy.
Perilesional biopsy represents a biologically rational strategy. Rather than sampling the entire prostate systematically, this approach focuses on the tissue immediately surrounding the MRI-visible lesion, typically within a defined margin of approximately 10 mm from the index target, where clinically significant cancer is most likely to extend beyond the visible lesion. By concentrating sampling in the area with the highest probability of tumour extension, perilesional biopsy may capture relevant disease while avoiding unnecessary systematic cores.
The TARGET trial is a prospective clinical study designed to directly compare these two diagnostic strategies in patients undergoing MRI-guided prostate biopsy. By evaluating whether targeted plus perilesional sampling can maintain the detection rate of clinically significant prostate cancer while reducing the number of biopsy cores required, the study seeks to provide evidence for a more efficient and patient-centred diagnostic approach.
The potential implications of this work extend beyond procedural optimization. As imaging technologies continue to improve, prostate cancer diagnostics are increasingly moving toward lesion-directed approaches, where MRI findings guide not only biopsy strategies but also clinical decision-making. Trials such as TARGET are therefore essential for determining how far this paradigm can be applied without compromising diagnostic safety.
If the perilesional strategy proves non-inferior to systematic sampling, the results could support a meaningful simplification of prostate biopsy protocols. Reducing the number of cores taken during biopsy may improve patient experience, decrease procedure-related morbidity, and simplify diagnostic pathways in centres increasingly reliant on MRI-guided pathways.
Ultimately, the TARGET trial addresses one of the central questions in modern prostate cancer diagnostics: whether systematic biopsy remains necessary in the MRI era or whether more focused, imaging-driven strategies can safely guide cancer detection. By directly evaluating this question in a prospective clinical framework, the study may contribute to defining a more precise and patient-centred biopsy pathway for men undergoing prostate cancer evaluation.
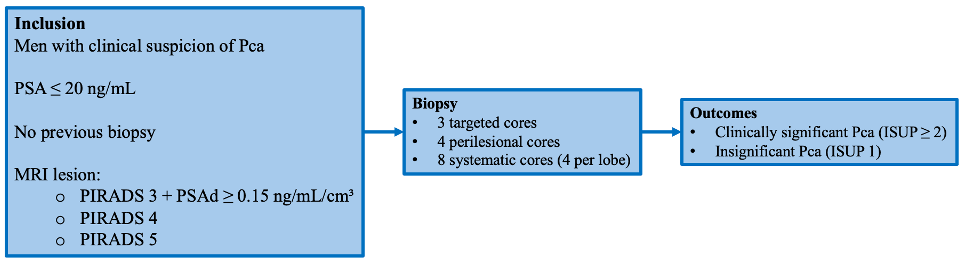
Figure 1. Study design of the TARGET trial
Written by: Federica Sordelli, Department of Urology, North Hospital, AP-HM, Aix-Marseille University, Marseille, France; Department of Biomedical Sciences, Humanitas University, Pieve Emanuele, Italy.
Read the Abstract