To better characterize contemporary practice, the URONCOR group (Urological Tumors Working Group of the Spanish Society of Radiation Oncology) conducted a national patterns-of-care survey exploring diagnostic strategies, radiotherapy approaches, systemic treatment, follow-up, and future perspectives in high-risk prostate cancer across Spain.
This survey collected responses from 74 radiation oncologists representing 71 hospitals—more than half of all radiotherapy centers nationwide—providing a comprehensive snapshot of current clinical practice. Most respondents worked in public university hospitals and reported substantial experience, with a median of 11 years in practice and approximately 50 high-risk prostate cancer patients treated annually per department.
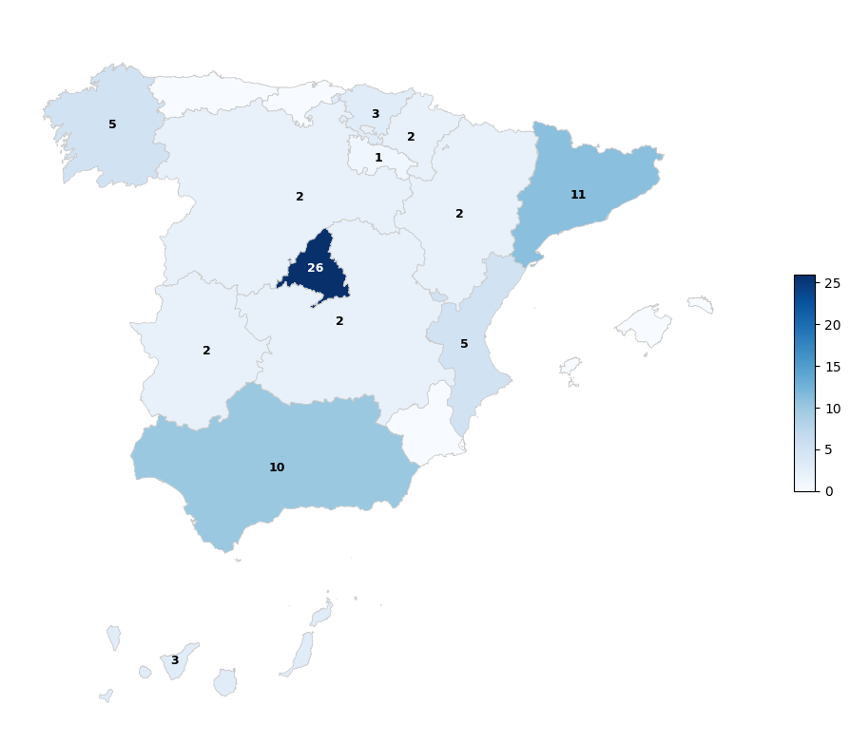
Figure 1. Number of participants per region.
Key Findings
Several important observations emerge from this national analysis.
First, radiotherapy practice is characterized by marked heterogeneity. A total of 26 distinct fractionation regimens were reported. Moderate hypofractionation has clearly become the dominant approach, while normofractionation has effectively disappeared from routine practice. Nevertheless, significant variability persists regarding dose schedules, planning margins, and boost strategies. Approximately 40% of centers combine external beam radiotherapy with brachytherapy boost, whereas stereotactic body radiotherapy remains limited to a minority of institutions.
Second, elective pelvic nodal irradiation in node-negative patients remains controversial in daily practice, with nearly equal proportions of centers performing whole-pelvis radiotherapy versus prostate-only treatment. This split mirrors the ongoing international debate following trials such as POP-RT and PIVOTAL, highlighting the absence of a unified clinical standard despite emerging phase III evidence.
Third, next-generation imaging is not yet universally adopted. Although PSMA-PET is strongly recommended by contemporary guidelines, only 28% of respondents reported its routine use for initial staging at the time of the survey. Importantly, this appears driven largely by reimbursement and access limitations rather than lack of clinical acceptance. With recent national reimbursement approval, wider implementation is anticipated.
From a systemic therapy perspective, long-term androgen deprivation therapy remains the backbone of treatment, with most centers prescribing 24 months of ADT. Notably, more than three-quarters of respondents reported incorporating abiraterone for very high-risk disease, reflecting rapid translation of evidence from the STAMPEDE platform into real-world practice.
Management of recurrence also demonstrates considerable variation. The majority of centers favor local salvage approaches following radiotherapy failure, primarily using HDR brachytherapy or Stereotactic Body Radiotherapy (SBRT). However, more than a dozen different salvage fractionation schedules were reported, underscoring the lack of standardized protocols in this setting.
Finally, future perspectives expressed by respondents reveal a clear shift toward personalized treatment strategies. Most clinicians favor individualized approaches guided by advanced imaging and genomic profiling, with additional interest in treatment intensification through androgen receptor pathway inhibitors and brachytherapy dose escalation. De-escalation strategies were supported by only a small minority.
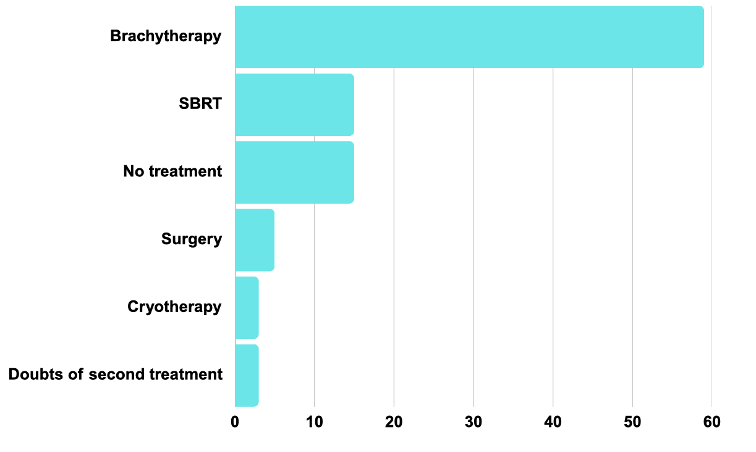
Figure 2. Treatment of local recurrence after prostate radiotherapy
Interpretation and Clinical Implications
Collectively, these findings highlight a transitional phase in the management of high-risk prostate cancer in Spain. Moderate hypofractionation and long-term ADT now form a common therapeutic foundation, while treatment intensification—both local and systemic—is increasingly embraced. At the same time, substantial variability persists across nearly every domain of care.
Importantly, several practice patterns appear driven more by structural factors than by scientific uncertainty. Limited access to PSMA-PET at the time of the survey illustrates how healthcare system constraints can delay implementation of evidence-based innovations. Conversely, the rapid uptake of abiraterone in very high-risk disease demonstrates the oncology community’s readiness to integrate high-level evidence when access is available.
The observed heterogeneity in radiotherapy techniques, pelvic nodal irradiation, and salvage strategies suggests that many clinical decisions remain institution-dependent rather than guideline-driven. While individualized care is essential, excessive variability may compromise equity and consistency of outcomes at a population level.
Methodological Considerations
This study has inherent limitations, including a response rate of approximately 32% and potential overrepresentation of high-volume academic centers. Nevertheless, participation from more than half of Spanish radiotherapy departments and representation from nearly all regions provide a robust overview of national practice patterns. As such, these results offer valuable insight into real-world management of high-risk prostate cancer within a European healthcare system.
Looking Forward: A Call for National Consensus
The URONCOR patterns-of-care survey reveals both progress and fragmentation in contemporary high-risk prostate cancer management. While advances in hypofractionated radiotherapy, systemic intensification, and salvage approaches are evident, the absence of harmonized treatment pathways remains striking.
These findings strongly support the need for national consensus guidelines that integrate modern imaging, genomic stratification, and risk-adapted therapeutic strategies. Collaborative efforts led by multidisciplinary groups such as URONCOR may play a pivotal role in standardizing care, promoting evidence-based decision-making, and ensuring equitable access to innovation across institutions.
Future research should focus on prospective validation of personalized treatment algorithms, optimization of pelvic irradiation strategies, integration of PSMA-guided planning, and refinement of salvage protocols. Ultimately, aligning clinical practice with emerging evidence will be essential to improving outcomes for patients with high-risk prostate cancer.
Written by: Victor Duque-Santana
- Department of Radiation Oncology, Hospital Universitario Quirónsalud Madrid. Madrid, España,
- Departamento de Medicina, Facultad de Medicina, Salud y Deportes, Universidad Europea de Madrid. Madrid, España