Our Spanish multicenter study, with a retrospective design and relatively short follow-up, provides relevant information on 2-year oncologic outcomes and late adverse events following stereotactic body radiotherapy. A total of 250 patients with localized prostate cancer treated across 12 Spanish centers between January 2020 and December 2023 were analyzed. Biochemical recurrence was defined according to the Phoenix criterion (PSA nadir + 2 ng/mL). Late genitourinary, gastrointestinal, and sexual adverse events were assessed using CTCAE v5.0. Univariate and multivariate analyses were performed to identify factors associated with outcomes, and survival was estimated using the Kaplan–Meier method with log-rank testing (p < 0.05).
The median age was 72 years (IQR: 65–76), and the median baseline PSA was 6.7 ng/mL (IQR: 5.3–8.7). According to NCCN risk classification, 30% of patients were low risk, 67% intermediate risk (26.8% favorable and 39.6% unfavorable), and 3% high or very high risk. The median prescribed dose was 40 Gy in five fractions (range: 36.25–40.0), delivered on alternate days. At 2 years, biochemical control reached 96.4%, and radiological progression was observed in 2.8% of patients, predominantly nodal. The incidence of late adverse events ≥ grade 2 was 7.6% genitourinary, 1.2% gastrointestinal, and 14.3% sexual, while grade 3 adverse events were infrequent (2.0% genitourinary, 0.8% gastrointestinal, and 3.8% sexual). These outcomes were achieved under standardized protocols including daily image guidance, reduced margins, urethral-sparing strategies, and systematic use of rectal spacers in most patients.
The high 2-year overall survival rate (95.6%), together with the absence of prostate cancer–specific mortality during the analyzed period, reflects effective 2-year disease control and the generally indolent natural history of localized prostate cancer in most included patients. These findings should not be interpreted as evidence of a cancer-specific survival benefit, but rather as expected outcomes in a predominantly low- and intermediate-risk cohort with limited follow-up. Nonetheless, they support the early oncologic safety of SBRT in this clinical setting.
The low rates of clinically relevant late adverse events (≥ grade 2) across genitourinary, gastrointestinal, and sexual domains confirm a favorable safety profile of SBRT in routine clinical practice when modern technical strategies are applied. The low frequency of grade 3 events suggests that severe adverse events are uncommon with contemporary SBRT regimens in appropriately selected patients. These data support the concept that dose intensification per fraction, when accompanied by strict planning, motion management, and adequate organ-at-risk protection, does not necessarily translate into a clinically meaningful increase in severe late adverse events. However, the retrospective design and relatively short follow-up limit the characterization of very late adverse events.
In summary, SBRT for localized prostate cancer offers a favorable balance between high 2-year oncologic control and an acceptable late adverse event profile in a multicenter real-world setting. When delivered in experienced centers with modern image guidance and robust quality assurance, SBRT can be considered a consolidated treatment option for appropriately selected patients. External validation and longer follow-up will be essential to confirm the durability of tumor control, long-term safety, and the true impact on cancer-specific survival.
Table. Incidence of late toxicities.
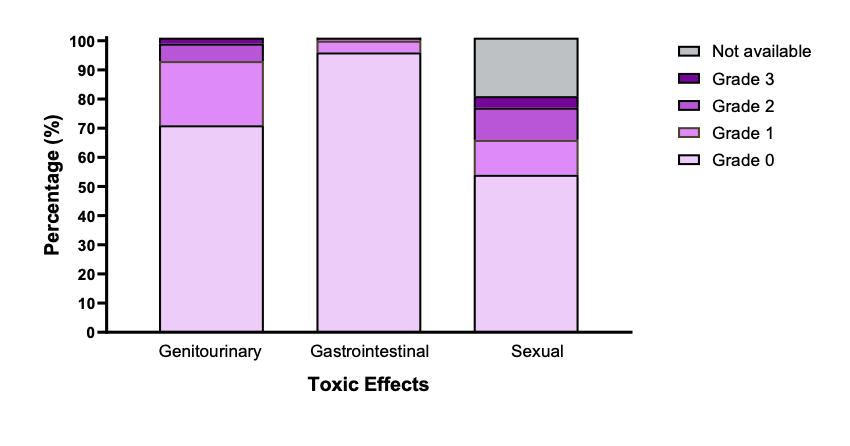
Distribution of chronic genitourinary (GU), gastrointestinal (GI), and sexual toxicities according to CTCAE v5.0. Data correspond to the highest-grade adverse event in each domain per patient. The incidence of grade ≥2 late GU, GI, and sexual toxicities was 7.6%, 1.2%, and 14.3%, respectively.

Figure. Conformal SBRT dose distribution in localized prostate cancer with urethral visualization.
Axial cross-sectional planning CT slice illustrating stereotactic body radiotherapy (SBRT) dose distribution for localized prostate cancer prescribed to 36.25 Gy in 5 fractions. The prostate planning target volume (PTV) is delineated by the red contour and demonstrates conformal high-dose coverage. The intraprostatic urethra is visible, and a fiducial marker is identified to support image-guided radiotherapy. The color wash represents the delivered dose in centigray (cGy), with warmer colors indicating higher doses (up to approximately 38.9 Gy) and cooler colors indicating lower doses, highlighting the steep dose gradients and dosimetric precision of SBRT while prioritizing urethral awareness and sparing.
Written by: Sigfredo Elias Romero Zoghbi, MD, Department of Radiation Oncology, GenesisCare Talavera de la Reina, Talavera de la Reina, Spain; Doctoral and Research School, Universidad Europea de Madrid, Madrid, Spain.
Read the Abstract