One of the major strengths of this trial is its multinational design. By enrolling 775 patients from 11 countries spanning Latin America, Europe, the Middle East, and Asia, the study moves beyond the traditional single-region evidence base that frequently shapes clinical practice. Instead, it captures real-world variability in patient populations, clinical workflows, and healthcare infrastructure. This geographic diversity strengthens the external validity of the findings and supports the broader generalizability of PSMA PET/CT as a prognostic tool.
The prospective methodology further reinforces the robustness of the conclusions. Patients underwent PSMA PET/CT after being classified as nonmetastatic on conventional imaging, enabling a direct evaluation of the incremental prognostic value of molecular imaging. Notably, PSMA-defined disease extent—PET N0M0 (no PET-detected nodal or distant disease), PET N1M0 (pelvic nodal involvement), and PET NxM1 (distant metastatic disease)—emerged as the only significant determinant of survival outcomes.
PSMA-detected N1M0 and NxM1 disease independently predicted worse event-free survival, even after adjustment for age, ISUP grade, high-risk status, and PSA level. More strikingly, metastatic disease identified on PSMA PET/CT was the sole predictor of overall survival, conferring nearly a 50-fold higher risk of death. Traditional clinical variables did not retain independent significance in multivariate analyses, underscoring a critical shift in risk assessment: whole-body molecular tumor distribution may be more informative than conventional clinicopathologic markers alone.
From a clinical perspective, the clear separation in event-free and overall survival among PET-defined groups highlights the transformative role of PSMA PET/CT in initial risk stratification. Patients with molecularly localized disease demonstrated excellent short-term survival, whereas those with distant metastases experienced substantially poorer outcomes. This degree of prognostic discrimination supports earlier treatment intensification for biologically aggressive disease while helping to avoid overtreatment in patients with truly localized tumors. In an era increasingly defined by precision oncology, imaging biomarkers that directly inform prognosis are indispensable.
Beyond its clinical implications, this study speaks to the growing democratization of advanced molecular imaging. Historically, access to cutting-edge nuclear medicine technologies has been uneven, constrained by infrastructure requirements and specialized expertise. The successful implementation of PSMA PET/CT across countries with varying resource levels demonstrates that global dissemination is achievable when supported by coordinated international frameworks. The IAEA has played a pivotal role in this process by fostering training, standardization, and technical cooperation—elements essential for ensuring consistency and scientific rigor in multicenter imaging trials.
Several limitations warrant consideration. The absence of a randomized comparator staged exclusively with conventional imaging prevents definitive quantification of survival benefits directly attributable to PSMA-guided management changes. Additionally, treatment heterogeneity across participating centers introduces clinical variability. However, this diversity arguably enhances the real-world relevance of the findings, reflecting the environments in which PSMA PET/CT is increasingly being integrated. A longer follow-up will be important to confirm whether the observed prognostic gradients persist over time.
The implications extend well beyond prostate cancer. This investigation provides a practical blueprint for future multinational imaging trials aimed at validating biomarkers capable of shaping therapeutic strategy. As theranostics and targeted radiopharmaceuticals continue to expand, collaborative research platforms—particularly those supported by independent intergovernmental organizations such as the IAEA—will be essential for generating evidence that is both scientifically rigorous and globally applicable.
Ultimately, the success of this IAEA-supported initiative reinforces a central principle: progress in cancer care depends not only on technological innovation but also on the strength of international partnerships that enable equitable access to those advances. PSMA PET/CT is no longer merely improving detection—it is redefining prognostic assessment and helping establish a more predictive, personalized, and globally connected model of oncologic care.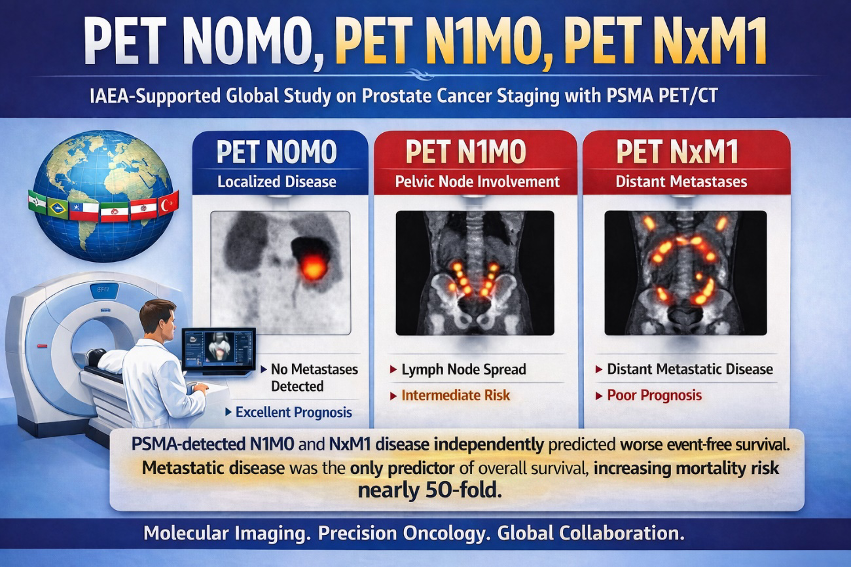
Written by: Juliano J. Cerci,1 Stefano Fanti,2 Enrique E. Lobato,3 Rakesh Kumar,4 Jolanta Kunikowska,5 Akram Al-Ibraheem,6 Maisarah Nasir,7 Francisca Redondo Moneda,8 Osvaldo Garcia,9 Mohamad Haidar,10 Fuad Novruzov,11 Ozlem Kucuk,12 Umut Elboga,13 Murilo de Almeida Luz,14 Diana Paez,3
- Quanta Diagnostico e Terapia, Curitiba, Brazil.
- IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy.
- Division of Human Health, International Atomic Energy Agency, Vienna, Austria.
- All India Institute of Medical Sciences, New Delhi, India.
- Nuclear Medicine Department, Medical University of Warsaw, Warsaw, Poland.
- King Hussein Cancer Center, Amman, Jordan.
- Institute Kanser Negara, Putrajaya, Malaysia.
- Asistencial Sotero del Río, Santiago Clínica Andes Salud, Puerto Montt, Chile.
- Instituto Nacional de Cancerologia, Tlalpan, Mexico.
- American University of Beirut Medical Center, Beirut, Lebanon.
- Nuclear Medicine Department, National Centre of Oncology, Baku, Azerbaijan.
- Ankara University, Ankara, Turkey.
- University of Gaziantep, Gaziantep, Turkey; and.
- Icahn School of Medicine at Mount Sinai, New York, New York.