In the Dutch MR PROPER trial, we examined how PSA-density thresholds influence the benefit-to-harm balance of MRI and biopsy decisions in a community-based setting on a national level. Among almost 1,000 men undergoing MRI and subsequent biopsy (if indicated), clinically significant cancer (GG≥2) was present in 24%. However, almost half of MRI positive findings (PI RADS ≥3) did not yield significant disease, highlighting the need for more selective upstream testing.
Our findings support two clinically relevant refinements.
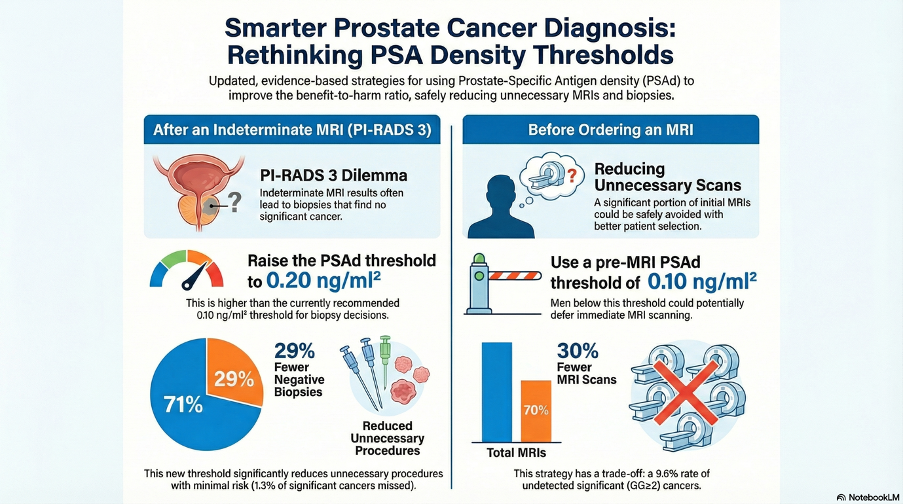
First, for biopsy indication, a post‑MRI PSA-density threshold of ≥0.20 ng/ml² in men with PI‑RADS 3 lesions substantially reduced safely unnecessary biopsies, avoiding 29% (38/133) of negative biopsies and 4% (3/84) of GG1 diagnoses, while missing only 1% (3/239) of all GG≥2 cancers. This threshold improved benefit‑to‑harm ratios across cancer‑averse and biopsy‑averse scenarios.
Second, for MRI indication, a pre‑MRI PSA-density threshold of ≥0.10 ng/ml² in all men substantially reduced 30% (301/996) MRI scans and potentially reduced 38% (50/133) of unproductive biopsies, at the cost of missing 1 in 10 GG≥2 cancers. This trade‑off may be acceptable in biopsy‑averse settings (e.g., population-based screening settings) with robust follow‑up pathways, as costs-savings are high (Figure 1).
Together, these results illustrate that the PSA-density biomarker can meaningfully enhance risk‑based MRI pathways, either by reducing unnecessary biopsies after MRI or by limiting upfront MRI use. At the proposed PSA-density thresholds at a prevalence of 24%, significant prostate cancer at a nation-wide level, we maintain oncological safety while achieving diagnostic efficiency. These data support a more nuanced, threshold‑adapted approach to MRI-based prostate cancer diagnostics, though future research should prospectively validate these results.
These insights may guide follow-up scenarios in different healthcare systems, balancing the risk of leaving small prostate cancers undetected and the overuse of diagnostic MRI scans or biopsies and subsequent overdiagnosis and overtreatment.
Written by: Anne Prinsen,1,2,3 Roderick van den Bergh,2 Ivo G. Schoots3
- Department of Urology, Sint Antonius Ziekenhuis, Nieuwegein, The Netherlands;
- Department of Urology, Erasmus University Medical Centre, Rotterdam, The Netherlands;
- Department of Radiology and Nuclear Medicine, Erasmus University Medical Centre, Rotterdam, The Netherlands.