The European Registry of Next-Generation Imaging in Advanced Prostate Cancer (RING) was created to address exactly these questions. RING is a non-interventional, investigator-initiated, multinational registry that captures real-world imaging pathways in men with prostate cancer at risk of having metastases, either at initial diagnosis or at biochemical relapse after local therapy.
The registry does not favor any imaging strategy; instead, it captures real clinical choices and analyses their impact on treatment decisions (Stage 1). Stage 2 of the Registry is designed to assess the link between different imaging pathways and survival outcomes.
Preliminary results - first 100 patients
For this Beyond the Abstract, we report our first real-world data from RING. Since January till July 2025, 8 European Centers were activated with 102 patients included, having sufficient data for this interim analysis. The cohort reflects the heterogeneity of advanced prostate cancer patients: the majority have undergone imaging workup at initial staging (70%), with the remainder at biochemical recurrence.
While all imaging strategies (CI, NGI, or a combination of both) are represented in the registry, the NGI-based pathway clearly predominates in naïve (70%) and specifically in recurrent patients (91%). It means that in daily practice, PSMA PET/CT is no longer reserved for exceptional scenarios - it is already the default imaging modality for many high-risk men.
A key question for us was who gets NGI in real life. Treatment naïve patients undergoing NGI are younger (p=0.04) and tend to have higher baseline PSA (p=0.06). Moreover, biopsy ISUP grade group ≥4 is strongly associated with NGI use (OR 5.1 (95% CI: 1.7-15.2, p=0.005)). This is an important detail: while the “high risk” definition incorporates PSA, grade group, and clinical stage, our early RING data suggest that in daily practice, clinicians weigh more tumor aggressiveness when deciding to escalate from CI to PSMA PET/CT.
Moreover, interim analysis demonstrates that NGI already drives treatment decisions when it is available (75% of treatment decisions were based on NGI results in treatment naïve patients and 90% - in BCR group).
Interesting outcomes come from the subgroup of patients who underwent both imaging modalities (n=19). First, some new data emerged for the phenomenon of “stage migration” with PSMA PET. In the RING, the dominant effect of PET/CT is not just “up-staging”, but rather the redistribution of patients with CI indeterminate results into either clearly PET-positive or PET-negative (reducing indeterminate results from roughly 60% to about 10%) (fig.1).
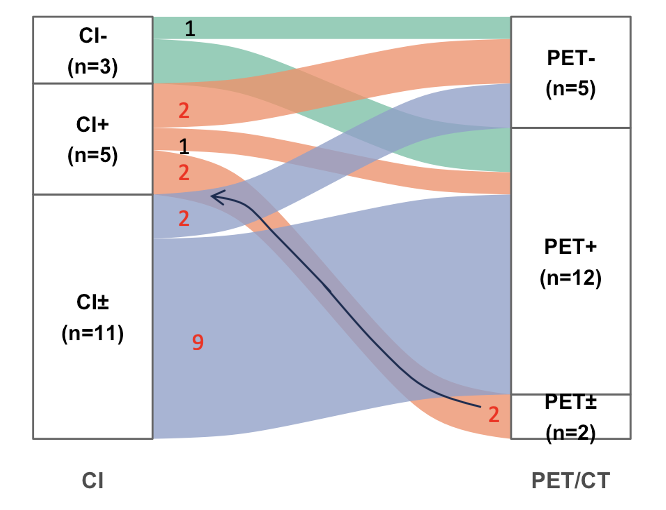
Fig.1 Alluvial plot demonstrating the reclassification of CI results with PSMA PET/CT imaging.
From this, we can suggest that the main clinical gain of PSMA PET/CT in prostate cancer nowadays is resolving uncertainty about metastatic status so that patients can be assigned to a clear M0 or M1 treatment pathway.
Several prospective trials have already established the diagnostic advantages of PSMA PET/CT and begun to explore its prognostic value. What has been missing is a real-world view of how different imaging workups are distributed in daily practice across Europe. The full RING data will allow us to assess this heterogeneity of imaging pathways in advanced prostate cancer patients and evaluate the impact of imaging not only on treatment decisions, but also on patient outcomes.
Written by: Daria Chernysheva,1 Stefano Fanti,2,3 Anders Bjartell,4 Luca Afferi,5 Alberto Breda,6 Joan Palou,6,7 Anwar R. Padhani,8 Francesco Sanguedolce,9,10
- Urooncology, Fundacio Puigvert Barcelona, Barcelona, Spain.
- IRCCS AOU Bologna, Bologna, Italy.
- University of Bologna, Bologna, Italy.
- Skåne University Hospital, Malmö, Sweden.
- Department of Urology, Luzerner Kantonsspital, Lucerne, LU, Switzerland.
- Fundacio Puigvert, Barcelona, Spain.
- Autonomous University of Barcelona, Barcelona, Spain.
- Mount Vernon Cancer Centre, Northwood, UK.
- Urology, Fundacio Puigvert, Barcelona, Barcelona, Spain
- Department of Medicine, Surgery and Pharmacy, Universita degli Studi di Sassari, Sassari, Sardinia, Italy.
- Prostate Cancer - Uroweb [Internet]. [cited 2025 Jun 10]. Available from: https://uroweb.org/guidelines/prostate-cancer/chapter/introduction
- Chow KM, So WZ, Lee HJ, Lee A, Wei D, Yap T, et al. Head-to-head Comparison of the Diagnostic Accuracy of Prostate-specific Membrane Antigen Positron Emission Tomography and Conventional Imaging Modalities for Initial Staging of Intermediate-to High-risk Prostate Cancer: A Systematic Review and Meta-analysis Positron emission tomography Systematic review Meta-analysis. [cited 2025 Apr 8]; Available from: https://doi.org/10.1016/j.eururo.2023.03.001
- Hofman MS, Lawrentschuk N, Francis RJ, Tang C, Vela I, Thomas P, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): a prospective, randomised, multicentre study. The Lancet. 2020 Apr 11;395(10231):1208–16.
- Morris MJ, Rowe SP, Gorin MA, Saperstein L, Pouliot F, Josephson D, et al. Diagnostic Performance of 18F-DCFPyL-PET/CT in Men with Biochemically Recurrent Prostate Cancer: Results from the CONDOR Phase III, Multicenter Study. Clin Cancer Res [Internet]. 2021 Jul 1 [cited 2025 Aug 4];27(13):3674–82.
- Pienta KJ, Gorin MA, Rowe SP, Carroll PR, Pouliot F, Probst S, et al. A Phase 2/3 Prospective Multicenter Study of the Diagnostic Accuracy of Prostate Specific Membrane Antigen PET/CT with 18F-DCFPyL in Prostate Cancer Patients (OSPREY). J Urol [Internet]. 2021 Jul 1 [cited 2025 Aug 4];206(1):52–61.
- Perera M, Papa N, Roberts M, Williams M, Udovicich C, Vela I, et al. Gallium-68 Prostate-specific Membrane Antigen Positron Emission Tomography in Advanced Prostate Cancer—Updated Diagnostic Utility, Sensitivity, Specificity, and Distribution of Prostate-specific Membrane Antigen-avid Lesions: A Systematic Review and Meta-analysis. Eur Urol. 2020 Apr 1;77(4):403–17.