However, given the limitations of re-staging imaging, sLND remained limited by a non-negligible rate of negative findings on final pathology.4 With the growing utilization of more accurate re-staging modalities such as prostate-specific membrane antigen (PSMA) PET scan,5 it has been proposed that this may also improve the accuracy of sLND by guiding surgeons in the dissection of truly positive nodes. The outcomes might even be further enhanced with intraoperative PSMA-sensitive probes, that is, radio-guided surgery (RGS). This implementation showed promising results,6,7 but whether it might improve oncologic outcomes of sLND as compared to template sLND remains unknown. For this reason, we tested the hypothesis that the surgical technique utilized for sLND (template vs. radio-guided surgery) might be associated with oncologic outcomes after sLND.
We retrospectively analyzed data of 339 patients with ≤2 pelvic lymph-node recurrence(s) of prostate cancer after radical prostatectomy documented on PSMA PET scan and treated with pelvic sLND at 11 institutions between 2012 and 2022.
No retroperitoneal lymph node dissections were included. Similarly, no patient with evidence of bone metastases was included. We excluded patients with PSA at sLND >4 ng/ml (n=35), who were on androgen-deprivation therapy at the time of PET scan (n=2), or who had missing covariates (n=43), resulting in 259 patients eligible for the analyses.
Patients were stratified in two groups according to the surgical strategy utilized for sLND, either template sLND or sLND using RGS. Template sLND included the bilateral excision of external iliac, obturator, internal iliac, common iliac, and presacral nodes.3,8,9 With respect to RGS, a gamma probe for open (Crystal Probe CXS-SG603; Crystal Photonics, Berlin, Germany) or robotic surgery (Drop-in probe CXS-OP-DP; Crystal Photonics, Berlin, Germany or SENSEI probe by Lightpoint, a Telix Pharmaceuticals Company, London, UK) was used. For radiolabelling 111In-PSMA-I&T, 99mTc-PSMA-I&S or 99mTc-MIP-1404 was used; there was no fluorescence labelling. In case of recurrent tumor within the extended pelvic lymph node dissection template, RGS was performed for the entire extended template of the affected side and, in some cases, also for the contralateral extended template if deemed necessary according to the surgeon’s discretion.6,7 In-vivo and ex-vivo measurements with a gamma probe were performed; if no elevated radioactivity was obtained on ex-vivo measurements (at least twice background), further resection and in-vivo measurements within the extended template were triggered. For suspicious lesions located elsewhere (e.g., pararectal), resection of the corresponding region with surrounding tissue was performed. Additional therapies after sLND included radiation and androgen deprivation therapy. Biochemical recurrence (BCR) was defined as PSA level ≥0.2 ng/ml and rising. Clinical recurrence (CR) was defined as positive imaging in the presence of a rising PSA in two consecutive measurements.
Kaplan-Meier curves assessed BCR- and CR-free survival rates, stratified by surgical technique. Multivariable Cox regression models assessed whether surgical technique was associated with BCR and CR after sLND. The adjustment for case-mix included the following variables that were selected a priori: International Society of Urological Pathology (ISUP) grade at radical prostatectomy, PSA level at sLND, age at sLND, number of nodes removed at sLND, number of positive nodes at sLND (0 vs. 1-2 vs. 3+), PSA response after sLND (continuous), and administration of additional therapies within 6 months after sLND (no vs. yes). This temporal window was chosen to reproduce a multi-modal treatment strategy delivered right after surgery, according to a previously defined cut-off10. Since data from different institutions are correlated, we incorporated institution clustering in our analysis using the cluster option in Stata statistical software. Finally, we performed sensitivity analyses to assess the robustness of our findings.
Overall, 80 (31%) and 179 (69%) patients in our cohort received template and radio-guided sLND, respectively (Table 1). While disease characteristics at radical prostatectomy did not differ between the groups, PSA level at sLND was higher in the template vs. radio-guided group (median: 1.3 vs. 0.6 ng/ml; p<0.0001). The distribution of positive spots on PSMA PET scan, total number of nodes removed, and positive nodes on sLND pathology did not differ between the groups (all p≥0.13). As compared to patients treated with template sLND, the first PSA after sLND was lower for those in the RGS group (median 0.1 vs. 0.5 ng/ml; p<0.0001). The rate of additional therapies after sLND was significantly higher in the template vs. RGS group (15% vs. 4%; p=0.003).
Table 1: Baseline characteristics of 259 patients with node-only recurrent prostate cancer on PSMA PET treated with radio-guided vs. template salvage lymph node dissection. All numbers are frequencies (proportions) and medians (interquartile range).
|
Template sLND (N=80; 31%) |
Radio-guided surgery (N=179; 69%) |
p |
|
|
ISUP group at RP |
|||
|
1 |
9 (11%) |
11 (6.1%) |
0.3 |
|
2 |
19 (24%) |
51 (28%) |
|
|
3 |
28 (35%) |
76 (42%) |
|
|
4 |
11 (14%) |
14 (7.8%) |
|
|
5 |
13 (16%) |
27 (15%) |
|
|
pT stage at RP |
|||
|
pT2 |
35 (44%) |
74 (41%) |
0.14 |
|
pT3a |
30 (38%) |
55 (31%) |
|
|
pT3b |
13 (16%) |
50 (28%) |
|
|
Unknown |
2 (2%) |
- |
|
|
pN stage at RP |
|||
|
pN0 |
53 (66%) |
143 (80%) |
0.022 |
|
pN1 |
8 (10%) |
27 (15%) |
|
|
pNx |
11 (14%) |
9 (5%) |
|
|
Unknown |
8 (10%) |
- |
|
|
Radiotherapy after RP |
45 (56%) |
101 (56%) |
0.10 |
|
Unknown |
14 (18%) |
- |
|
|
Age at sLND, yr |
68 (62, 71) |
66 (60, 70) |
0.15 |
|
PSA at sLND, ng/ml |
1.3 (0.7, 2.3) |
0.6 (0.3, 1.2) |
<0.0001 |
|
Number of positive PET spots |
|||
|
1 |
62 (78%) |
136 (76%) |
0.8 |
|
2 |
18 (22%) |
43 (24%) |
|
|
Number of nodes removed at sLND |
10 (5, 22) |
13 (8, 19) |
0.2 |
|
Number of positive nodes at sLND |
|||
|
0 |
23 (29%) |
46 (26%) |
0.3 |
|
1-2 |
43 (54%) |
86 (48%) |
|
|
3+ |
14 (18%) |
47 (26%) |
|
|
First PSA after sLND |
0.5 (0.1, 1.4) |
0.1 (0.0, 0.3) |
<0.0001 |
|
First PSA after sLND <0.1 ng/ml |
17 (21%) |
96 (54%) |
<0.0001 |
|
Additional therapies after sLND |
12 (15%) |
8 (4%) |
0.003 |
Abbreviations: sLND, salvage lymph node dissection; RP, radical prostatectomy
Overall, there were 181 biochemical recurrences and 76 clinical recurrences after sLND. Median follow-up for survivors in the template vs. RGS group was 7 (interquartile range [IQR]: 2, 17) vs. 24 (IQR: 12, 41) months, respectively. The 2-year BCR-free survival for patients in the template vs. RGS sLND was 18% (95% confidence interval [CI]: 9%, 29%) and 30% (95%CI: 22%, 37%), respectively. The 2-year CR-free survival for template vs. RGS sLND was 51% (95%CI: 35%, 65%) and 73% (95%CI: 65%, 80%; Figure 1), respectively.On multivariable analyses, we did not find evidence of a statistically significant difference for BCR after sLND between patients treated with template vs. RGS sLND (hazards ratio [HR]: 1.15; 95%CI: 0.57, 2.33; p=0.7). As compared to men who received a template sLND, those treated with RGS had a lower risk of clinical recurrence (HR: 0.51; 95%CI: 0.29, 0.92; p=0.026). Results of the sensitivity analyses were generally consistent with our main findings.
Our study suggests that men receiving sLND with radio-guided surgery might have better oncologic outcomes than those undergoing traditional template sLND. These findings may have several explanations.
Although surgical innovations are often appealing, what has the potential to establish a new standard of care is ultimately determined by improvement of outcomes. While many implementations in the field of urologic surgery showed promising results, their widespread adoption was often limited by the lack of relevant changes in outcomes. Radio-guided surgery for node-recurrent prostate cancer could probably be perceived as one of those. Now, our data suggests that RGS might not only represent an innovative solution for surgeons but might also improve outcomes of patients treated with sLND. This might be a consequence of the advantages offered to the operating surgeon, such as the possibility to modify the surgical template in case of additional positive findings in adjacent tissue – especially during immediate ex vivo measurements – or to continue surgical dissection in case of a negative signal by gamma probe measurements. That said, these results should also be commensurate with the short follow-up of our study, as we previously found that long-term outcomes of sLND might be suboptimal.3 Another possible limitation pertains to the administration of adjuvant treatment that, given the multi-institutional nature of our study, might have differed between centers. However, this parameter was included in our multivariable adjustment, and the results of sensitivity analyses after the exclusion of patients who received additional treatments after sLND were consistent with our main findings. The retrospective nature of our study represents another limitation, resulting in possible unmeasured confounding. For instance, the fact that template sLND was performed at different centers may have translated into different lymph node yields on final pathology. To address the issue, we have run sensitivity analyses including the number of lymph nodes removed on sLND, with no difference from our main results. We have also investigated whether baseline characteristics were different between men with available vs. missing covariates, with no significant discrepancy. Finally, we have to acknowledge that, for some men in the RGS group, resection was extended to non-regional lymph nodes (e.g., para-rectal), raising concerns for selection bias. Yet our data suggested better clinical recurrence-free survival for patients in the RGS vs. template sLND group. As for prior papers,10 any selection bias in the study would operate in the opposite direction to our findings and, as such, we are positive that this factor did not significantly affect our findings.
In conclusion, our data suggest that, in candidates for salvage lymph node dissection for node-only recurrent prostate cancer, RGS might offer an important surgical guidance for surgeons, and this may eventually translate to improved oncologic outcomes. Awaiting further evidence on long-term outcomes of radio-guided surgery, our data represents the first multi-centric comparative evidence on different techniques for sLND, and provides relevant data for counselling patients with node-only recurrent prostate cancer.
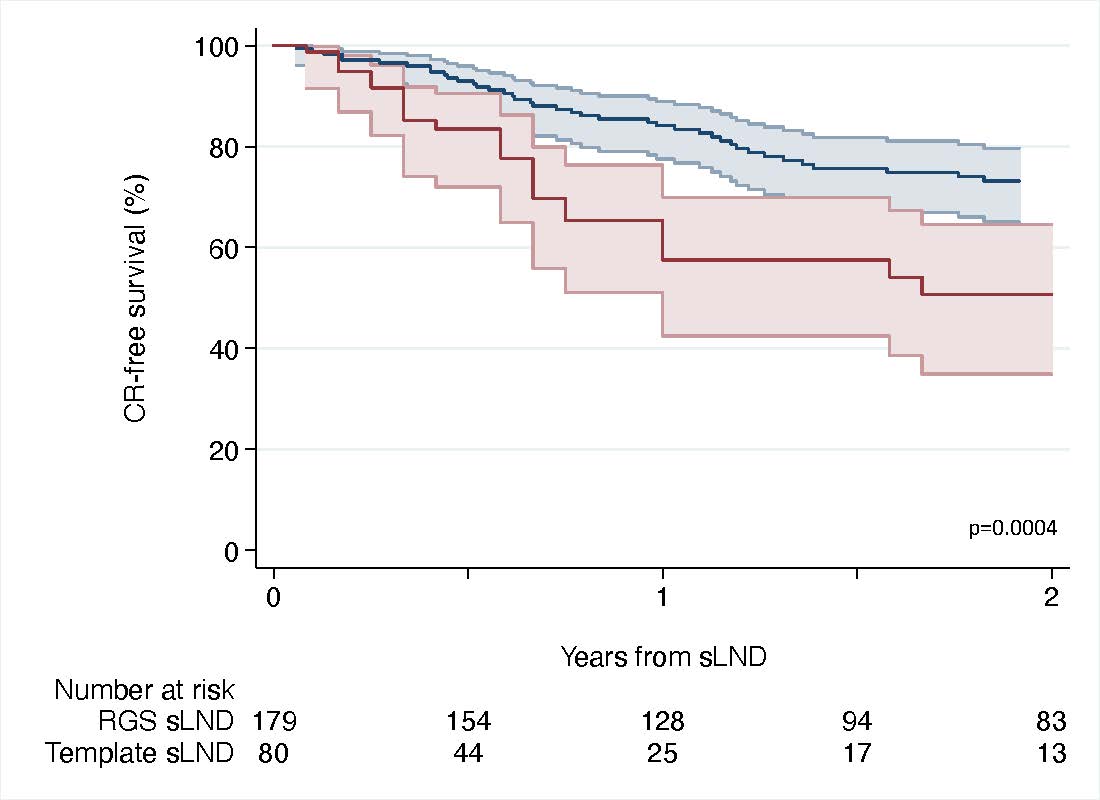
Figure 1. Kaplan-Meier curve assessing clinical recurrence-free survival (and 95% confidence interval) between template vs. radio-guided sLND for 259 patients with node-only recurrent prostate cancer documented on PSMA PET scan. Blue: radio-guided sLND. Red: Template sLND. P-value from log-rank test: 0.0004.
Written by: C.A. Bravi,1,2,3,4* S. Knipper,5,6* A. Heidenreich,7,8 N. Fossati,9 G. Gandaglia,4 P. Dell’Oglio,10,11,12 N. Suardi,13 D. Osmonov,14 K.P. Juenemann,14 R.J. Karnes,15 A. Kretschmer,16 L. Budäus,5 F. Falkenbach,5 A. Buchner16, C. Stief,16 A. Hiester,18 P. Albers,18 G. Devos,19 S. Joniau,19 H. Van Poppel,19 B. Grubmüller,20 S. Shariat,20,21 D. Pfister,7 D. Tilki,5 M. Graefen,5 I.S. Gill,22 A. Mottrie3, F. Montorsi,4 A. Briganti,4 T. Maurer5,23
- Department of Urology, Northampton General Hospital, Northampton, United Kingdom
- Department of Urology, The Royal Marsden NHS Foundation Trust, London, United Kingdom
- Department of Urology, Onze-Lieve-Vrouwziekenhuis Hospital, Aalst, Belgium
- Division of Oncology/Unit of Urology; URI; IRCCS Ospedale San Raffaele, Milan, Italy
- Martini-Klinik Prostate Cancer Center, University Hospital Hamburg-Eppendorf, Hamburg, Germany
- Department of Urology, Vivantes Klinikum am Urban, Berlin, Germany
- University of Cologne, Department of Urology, Cologne, Germany
- Dept. of Urology, Medical University Vienna, Austria
- Department of Urology, Ospedale Regionale di Lugano, Civico USI - Università della Svizzera Italiana, Lugano, Switzerland
- Department of Urology, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy.
- Department of Urology, Netherlands Cancer Institute-Antoni Van Leeuwenhoek Hospital, Amsterdam, The Netherlands.
- Interventional Molecular Imaging Laboratory, Department of Radiology, Leiden University Medical Center, Leiden, The Netherlands.
- Department of Urology, Ospedali Civili of Brescia, Brescia, Italy
- University Hospital Schleswig Holstein, Department of Urology and Pediatric Urology, Campus Kiel, Germany
- Mayo Clinic, Department of Urology, Rochester, Minnesota, United States
- Ludwig-Maximilians-University, Department of Urology, Munich, Germany
- Universitätsklinikum des Saarlandes, Homburg
- Department of Urology, Medical Faculty, Heinrich-Heine-University, Düsseldorf, Germany
- University Hospitals Leuven, Department of Urology, Leuven, Belgium
- Department of Urology, Medical University of Vienna, Vienna, Austria
- Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
- University of Southern California, USC Institute of Urology, Los Angeles, California, USA
- Department of Urology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- Ploussard G, Gandaglia G, Borgmann H, et al. Salvage Lymph Node Dissection for Nodal Recurrent Prostate Cancer: A Systematic Review. European Urology. October 2018:1-12. doi:10.1016/j.eururo.2018.10.041.
- Fossati N, Suardi N, Gandaglia G, et al. Identifying the Optimal Candidate for Salvage Lymph Node Dissection for Nodal Recurrence of Prostate Cancer: Results from a Large, Multi-institutional Analysis. European Urology. October 2018:1-8. doi:10.1016/j.eururo.2018.09.009.
- Bravi CA, Fossati N, Gandaglia G, et al. Long-term Outcomes of Salvage Lymph Node Dissection for Nodal Recurrence of Prostate Cancer After Radical Prostatectomy: Not as Good as Previously Thought. European Urology. July 2020:1-9. doi:10.1016/j.eururo.2020.06.043.
- Fossati N, Scarcella S, Gandaglia G, et al. Underestimation of PET/CT Scan in Assessing Tumour Burden of Men With Nodal Recurrence From Prostate Cancer: Head-to-Head Comparison of 68Ga-PSMA and 11C-Choline in a Large, Multi-Institutional Series of Extended Salvage Lymph Node Dissections. Journal of Urology. August 2020. doi:doi.org/10.1097/JU.0000000000000800.
- Maurer T, Eiber M, Schwaiger M, Gschwend JE. Current use of PSMA–PET in prostate cancer management. Nature Publishing Group. March 2016:1-10. doi:10.1038/nrurol.2016.26.
- Knipper S, Irai MM, Simon R, et al. Cohort Study of Oligorecurrent Prostate Cancer Patients: Oncological Outcomes of Patients Treated with Salvage Lymph Node Dissection via Prostate-specific Membrane Antigen-radioguided Surgery. European Urology. June 2022:1-8. doi:10.1016/j.eururo.2022.05.031.
- Knipper S, Tilki D, Mansholt J, et al. Metastases-yield and Prostate-specific Antigen Kinetics Following Salvage Lymph Node Dissection for Prostate Cancer: A Comparison Between Conventional Surgical Approach and Prostate-specific Membrane Antigen-radioguided Surgery. European Urology Focus. 2019;5(1):50-53. doi:10.1016/j.euf.2018.09.014.
- Bravi CA, Droghetti M, Fossati N, et al. Definition and Impact on Oncologic Outcomes of Persistently Elevated Prostate-specific Antigen After Salvage Lymph Node Dissection for Node-only Recurrent Prostate Cancer After Radical Prostatectomy: Clinical Implications for Multimodal Therapy. European Urology Oncology. June 2021:1-11. doi:10.1016/j.euo.2021.06.003.
- Bravi CA, Fossati N, Gandaglia G, et al. Assessing the Best Surgical Template at Salvage Pelvic Lymph Node Dissection for Nodal Recurrence of Prostate Cancer After Radical Prostatectomy: When Can Bilateral Dissection be Omitted? Results from a Multi-institutional Series. European Urology. July 2020:1-4. doi:10.1016/j.eururo.2020.06.047.
- Touijer KA, Karnes RJ, Passoni N, et al. Survival Outcomes of Men with Lymph Node-positive Prostate Cancer After Radical Prostatectomy: A Comparative Analysis of Different Postoperative Management Strategies. European Urology. 2018;73(6):890-896. doi:10.1016/j.eururo.2017.09.027.