Neuroendocrine differentiation in the prostate reflects the biology of scattered neuroendocrine cells that normally regulate glandular function. Under the pressure of AR pathway suppression or additional genetic events, prostate cancer cells adopt alternative lineage programs. Several mechanisms drive this process. Loss of AR expression, often associated with TMPRSS2::ERG fusions and AR gene alterations, is a hallmark of NEPC, though tumors may still retain low-level AR activity through splice variants or ligand-independent signaling.
Inactivation of tumor suppressors such as RB1, TP53, and PTEN accelerates lineage plasticity, often via SOX2 and E2F activation. Concurrently, amplification of oncogenes like NMYC and AURKA promotes stabilization of neuroendocrine phenotypes and correlates with aggressive clinical progression. Transcription factors such as ASCL1, NEUROD1, and FOXA2 orchestrate neuroendocrine gene programs, while epigenetic regulators, including EZH2 and LSD1, rewire the chromatin landscape, silencing AR-driven pathways and reinforcing neuroendocrine states. These molecular events underpin the aggressive biology and therapy resistance of NEPC.
Diagnosis rests on the integration of morphology, immunohistochemistry (IHC), and clinical context. SCNEC is often recognizable morphologically by features such as nuclear moulding, diffuse sheets of small cells, high mitotic rates, necrosis, and apoptotic bodies, while LCNEC often exhibits an organoid, trabecular, or palisading manner with more abundant amphophilic cytoplasm and tumor nuclei with coarse, clumpy chromatin, prominent nucleoli, frequent geographic necrosis, and brisk mitotic rate. IHC for neuroendocrine markers such as synaptophysin, chromogranin, and CD56 supports the diagnosis but lacks specificity since focal positivity may occur in conventional adenocarcinoma. In such cases, prostate-specific markers like NKX3.1, PSA and AR confirm tissue of origin, while proliferation indices such as Ki-67 appear to play a role in NEPC, with NEPCs exhibiting a significantly higher Ki-67 proliferative index (>50%) compared to conventional high-grade PC. The application of IHC is most useful when guided by clinical suspicion, such as in rapidly progressive disease, atypical visceral metastases, low PSA relative to disease burden, or negative PSMA scans in castration-resistant prostate cancer. Standardized reporting that incorporates morphology, AR, and neuroendocrine marker status, proliferation index, and clinical context is increasingly encouraged.
Clinically, neuroendocrine prostate cancers present with aggressive features, including visceral and lytic bone metastases, bulky tumor burden, rapid progression, and disproportionally low PSA levels. Their prognosis is poor, with a relatively shorter median survival for SCNEC and LCNEC. Even mixed adenocarcinoma-neuroendocrine tumors, which retain partial AR activity, remain highly aggressive and resistant to conventional hormone-directed therapies.
Management relies primarily on systemic therapy. Platinum-based chemotherapy, often with etoposide or taxanes, remains the backbone of treatment, producing initial responses but limited durability. Immunotherapy using checkpoint inhibitors such as nivolumab, ipilimumab, pembrolizumab, or atezolizumab is under investigation, though results so far have been modest. Molecularly targeted therapies are being explored, with inhibitors of AURKA showing activity in NMYC-amplified cases, and DLL3-targeted antibody–drug conjugates, bispecific T-cell engagers, and CAR-T therapies entering trials. Epigenetic regulators such as EZH2 and LSD1 represent additional therapeutic targets, and agents against novel surface molecules, including CD46, TROP2, NCAM1, and CXCR2, are under evaluation for both imaging and therapy. Advances in nuclear medicine offer further promise: FDG PET highlights aggressive biology, somatostatin receptor imaging provides diagnostic and potential therapeutic opportunities, and novel tracers such as glypican-3 ligands are being developed for theranostic approaches.
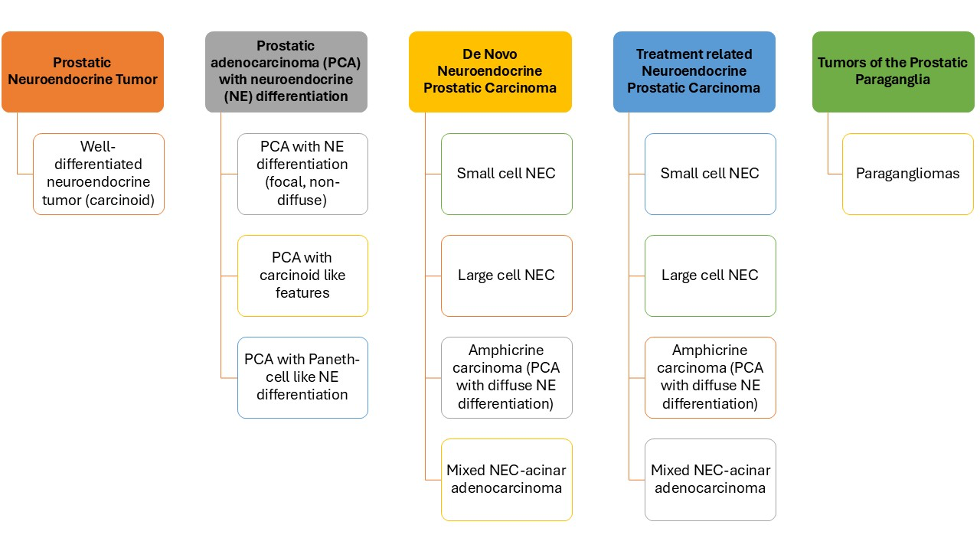
Given the limitations of existing frameworks, a prostate-specific classification system has been proposed that distinguishes adenocarcinoma with focal neuroendocrine differentiation, high-grade neuroendocrine carcinomas (SCNEC, LCNEC, mixed, and amphicrine), and rare paragangliomas of the prostate, while stratifying tumors by clinical setting (de novo versus treatment-related). Such an integrated model emphasizes morphology, immunoprofile, and clinical context to provide more meaningful prognostic and therapeutic guidance.
Future directions in this field include the integration of liquid biopsy approaches such as circulating tumor DNA analysis and methylation profiling, which allow real-time monitoring of treatment response, early detection of resistant clones, and identification of actionable alterations without invasive sampling. Molecular profiling of tumors is expected to refine classification, facilitate patient selection for targeted therapies, and enable precision oncology approaches. Prospective clinical trials are urgently needed to validate emerging targeted and immunotherapeutic strategies. Furthermore, theranostic approaches that combine molecular imaging with targeted radionuclide therapy hold particular promise in improving outcomes.
In conclusion, prostatic neuroendocrine tumors are a rare but highly aggressive spectrum of prostate cancers whose biology is shaped by AR suppression, tumor suppressor loss, oncogene activation, transcriptional reprogramming, and epigenetic plasticity. Current classification systems remain inadequate to capture their diversity, necessitating a prostate-specific model that integrates morphology, molecular features, and clinical setting. Advances in molecular diagnostics, liquid biopsy, targeted therapies, immunotherapy, and theranostics are beginning to open new therapeutic avenues. A shift toward molecularly informed classification and management offers the best chance of improving stratification, treatment selection, and survival in this challenging group of tumors.
New proposed classification for the neuroendocrine neoplasms of the prostate gland. (Lobo & Cheng)
Written by: Anandi Lobo, MD,1 and Liang Cheng, MD, MS,2
- Department of Pathology and Laboratory Medicine, Kapoor Center for Pathology and Urology, Raipur, India.
- Department of Pathology and Laboratory Medicine, Department of Surgery (Urology), Brown University Warren Alpert Medical School, the Legorreta Cancer Center at Brown University, and Brown University Health, Providence, RI, USA.
Read the Abstract