MRI prior to biopsy is now well established as a way to reduce unnecessary biopsies in men with raised prostate-specific antigen (PSA). But could MRI play an even more central role, serving as a first-line screening test in itself?
In this population-based study, we screened 303 men with an abbreviated biparametric MRI protocol consisting of axial T2-weighted imaging and high b-value (b2000) diffusion-weighted imaging. MRI was interpreted with a double-reader approach, with a third reader to resolve discrepancies. Men with a positive screening MRI or elevated PSA density (≥0.12 ng/mg2) were referred for standard-of-care investigations, including multiparametric MRI (mpMRI) and, if indicated, biopsy.
The prevalence of clinically significant PCa (Grade Group ≥2) was 9.6%. The screening MRI detected twice as many men with clinically significant PCa as PSA density, without increasing the detection of insignificant disease. Its positive predictive value (PPV) – i.e. the proportion of men with a positive screening MRI who were subsequently diagnosed with clinically significant PCa – was 59%. Among men with a positive screening MRI who were recommended for biopsy after mpMRI, the PPV rose to 86%. In practical terms, this translates to just over 1 in 10 unnecessary biopsies – far fewer than the ~1 in 2 unnecessary biopsies typically seen when mpMRI is used in standard diagnostic pathways.1
Why the difference? Our study effectively used a “stage-gated” approach: abbreviated biparametric MRI first, followed by mpMRI in screen-positive cases. This initial step drives up the disease prevalence in the men referred for mpMRI and raises the PPV. Interestingly, while the additional sequences at the mpMRI stage do provide further discrimination, presenting radiologists with all sequences upfront does not confer the same benefit. Could it be that less really is more?
This has important implications. When the harms and costs of follow-up investigations, such as biopsy, are significant, reducing false positives is critical. Counterintuitively, limiting information at the first step may actually improve radiologists’ discrimination, leading to more efficient and safer screening. The ultimate success of PCa screening may depend less on detecting small volume or MRI-invisible disease, and more on reliably identifying MRI-visible cancers with a high risk of progression at an earlier stage, with fewer unnecessary biopsies. While we have a tendency to seek as much information as possible, perhaps the way forward here is to work smarter, not harder.
Our current research builds directly on this insight. We are now investigating whether a “stage-gated” reporting approach could be applied to the interpretation of a single scan, where radiologists first review limited sequences and only review the remaining sequences if initial findings are positive (Figure 1). This may offer a pragmatic strategy towards scalable PCa screening which optimises both benefits and harms.
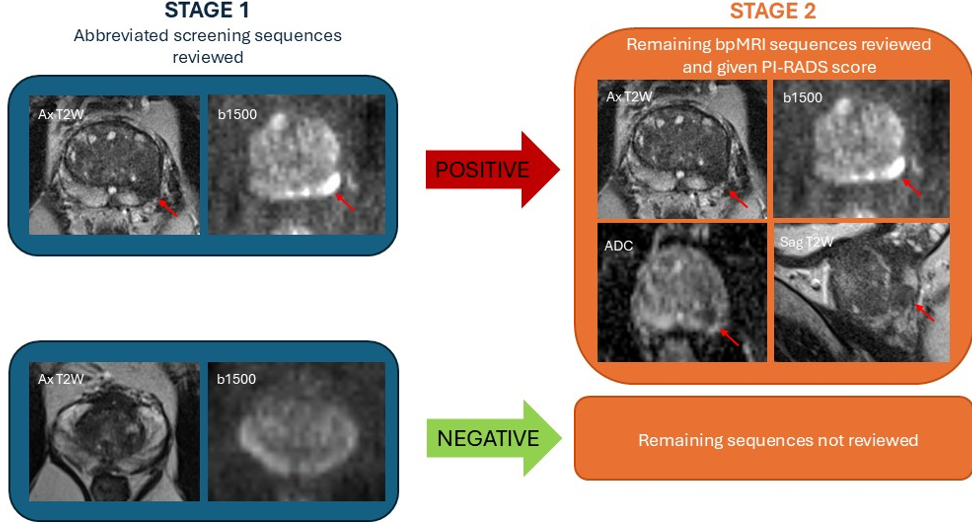
Figure 1: The “stage-gated” reporting approach
Written by: Natasha Thorley and Shonit Punwani, Centre for Medical Imaging, UCL, London, UK
Reference:
Read the Abstract