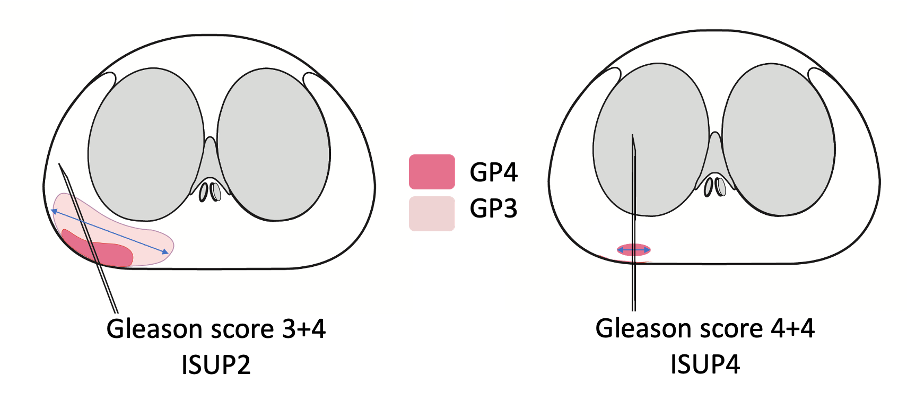
Figure 1: Illustration of Gleason scoring limitations. The left tumor (3+4, ISUP 2) has a higher metastatic risk than the right tumor (4+4, ISUP 4) because of a larger absolute GP4 volume, highlighting the value of quantifying GP4 burden
We analyzed a monocentric cohort of 446 men with ISUP 2–4 prostate cancer containing GP4 but no GP5, treated between 2009 and 2018. GP4 was quantified by three methods: percentage of GP4, length in millimeters, and MRI-derived and targeted biopsy-derived volume. We compared these against established risk tools (Gleason score, CAPRA, STAR-CAP, NCCN, and EAU).
Across all methods, GP4 quantification outperformed Gleason score and established risk scores in predicting recurrence and metastasis. MRI-estimated GP4 volume provided the highest discrimination, with a C-index of 0.80.
Our findings support incorporating GP4 burden—particularly MRI-derived volume—into routine risk stratification, offering a more precise and clinically relevant measure to guide treatment intensification or de-escalation.
Written by: Jonathan Olivier, MD, PhD, Urology Department, Claude Huriez Hospital, CHU Lille, Lille, France.
Read the Abstract