While PET/CT is widely known for its use in a wide variety of cancers for staging and follow-up using a radiolabeled molecule of fluorodeoxyglucose (FDG), a glucose analogue that is irreversibly trapped in the cancer cells, 18F-PSMA PET/CT is a more recent nuclear medicine imaging technique used mostly for detecting and staging prostate cancer. Instead of using the positron-emitting isotope 18F to label a molecule of FDG, it is used to label the prostate-specific membrane antigen (PSMA) molecule, which is then taken by the prostatic cancer cells that are overexpressing the receptor for this antigen. This allows for the detection of small lesions not detectable by other conventional imaging methods in the prostate, regional and extra-regional lymph nodes, and bones or viscera (Fig. 1). Alternatively, the study can also be performed using the isotope 68Ga, which has a shorter half-life than 18F (approximately 68 vs 110 minutes, respectively). Other tracers have been used to evaluate prostate cancer patients (i.e., choline, FLT, etc.),1,2 but it has been PSMA the one that has gained wide acceptance, given its higher diagnostic performance3 and its limited physiological uptake by most other organs (Fig. 2), which also allowed for targeted radioligand therapy (PRRT).4
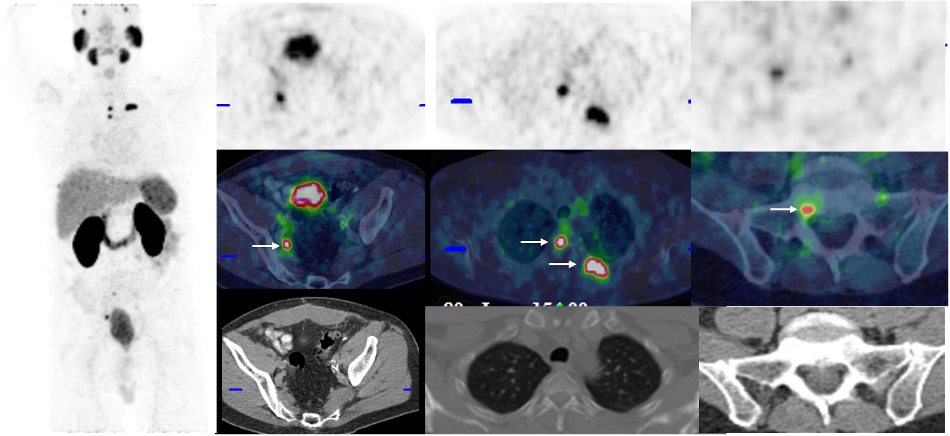
Figure 1 - History of radical prostatectomy 3 years ago (Gleason 7 (4+3), pT3a, N0; negative margins. Currently with biochemical recurrence (Serum PSA, 1.18 mcg/L). Patient underwent PSMA PET/CT, which showed lymph node recurrence in the right external iliac chain and at least 4 metastatic deposits in the bones (white arrows): two in the thoracic spine, one in the left 4th rib, and one in the vertebral body of S1.

Figure 2 - PSMA PET/CT with maximum intensity projection (MIP) reconstruction and CT, fusion, and PET images, respectively, at the level of the liver and spleen and at the level of the renal hilum bilaterally (Blue arrows on MIP). Usual distribution of the radiotracer is visualized in the MIP with uptake in the lacrimal, parotid, and submandibular glands, liver, spleen, kidneys, and excretory system, and some of the bowel (dotted blue arrow).
Why being good at detecting disease is relevant?
As shown in the PREP Registry study data and through other studies of PSMA PET/CT, this imaging will influence changes in management for a majority of men. What was less clear is whether these changes result in improved clinical outcomes for men. At the current time, there is a paucity of randomized controlled trials that demonstrate overall clinical benefit for PET-directed management of prostate cancer. The EMPIRE-1 study of Fluciclovine PSMA PET/CT did demonstrate improved biochemical control for men being considered for salvage radiotherapy for biochemical failure after radical prostatectomy, suggesting improved disease characterization translates into improved clinical outcomes.5 Similarly, the ongoing PATRON (NCT04557501) study, a Canada-wide study comparing standard of care therapy vs. PSMA PET/CT informed care among high-risk primary and recurrent prostate cancer, will help characterize potential benefits.6
The PREP Registry Study
The PSMA-PET Registry for Recurrent Prostate Cancer (PREP) study (NCT03718260) is a prospective study conducted in 6 academic hospitals across Ontario, Canada, and funded by the Cancer Care Ontario (Ontario Ministry of Health) that began in 2018, seeking to improve our ability to characterize patterns of recurrence and personalize therapies among men with suspected recurrence after primary therapy. At the time this registry study was initiated, no Health Canada-approved PSMA PET/CT tracers were available, and PREP was designed to acquire real-world evidence on the use of these novel PSMA PET/CT tracers while providing access under a Health Canada investigational new drug clinical trials authorization. PREP was initiated among men with suspected biochemical recurrence using the tracer 18F-DCFPyL. Successive iterations of the registry study have been expanded to include other disease scenarios (like primary high-risk staging and characterization of castrate resistant prostate cancer being assessed for peptide receptor radionuclide therapy (PRRT) and other tracers (18F-PSMA 1007). As the PREP study has evolved, ongoing analyses have provided insights as to the utility of PSMA PET/CT as deployed in Ontario.7,8
During the first phase of the PREP trial,8 spanning from 2018 to 2020, findings showed that 18F-PSMA PET/CT outperformed conventional imaging (CI: CT and 99mTc-methylene diphosphonate bone scan) in the detection of recurrent disease, particularly at low PSA levels. The second phase of PREP from 2020-2022 expanded indications to include failure after primary radiation and waived the necessity for CI in low yield groups (PSA <10 at time of imaging). In the second phase, which included those patients recruited during the first phase and new patients recruited between 2020 and 2022, findings showed that PET/CT-driven management change and pattern of metastatic spread in the said imaging study were linked to overall survival alongside the patient's clinical scenario. The latter corresponded to one of six cohorts (1-6) to which the patients were assigned depending on their initial treatment and stage of the disease (Table 1). Additionally, we saw no shift in the patterns of disease detected (loco-regional vs. limited metastatic vs. extensive metastases), suggesting that omission of the CI did not result in a shift in the types of recurrence detected.
Table 1 Study Cohorts*
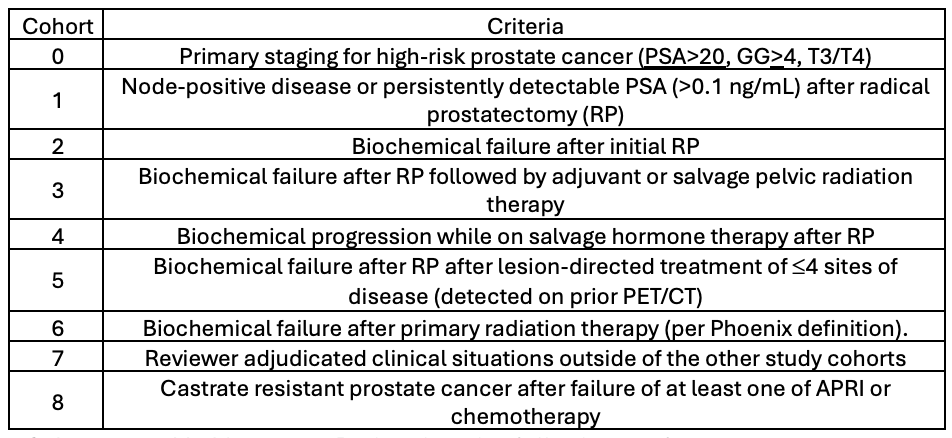
*Cohorts 0,8 added for current Registry iteration (effective 2023)
In the PREP Registry study, participants also consented to data linkage to the province of Ontario administrative health databases. Such linkages allowed for the correlation of PSMA PET/CT utilization with socioeconomic determinants of health, as well as the correlation of management changes following PSMA PET and patterns of disease recurrence with overall survival.9 As shown in the results combining the first and second phases of PREP,7 identification of recurrent sites of disease and proper delineation of it in or outside the pelvis changed patient management in a way that impacted overall survival (OS) independently in certain subgroups of patients. For example, while the study showed that management change after the use of PET/CT improved OS (Hazard Ratio of 0.6) in the overall population of the study, this only held true for patients in cohorts 4 and 6 (HR 0.4) and not for cohorts 2 and 3 (p=0.59) when performing a sub-analysis. Of note, management change from active therapy to observation was seen in only 9.5% (196/2070) of the population included, where 55% (105/196) of those changes happened after a negative PET/CT in patients most likely belonging to cohorts 2 and 3 as they represented the overwhelming majority of negative studies (82.2%; 176/214). The latter could help explain why management change had no significant impact on OS for cohorts 2 and 3, as management change by PET/CT was grouped, no matter the direction of change, and the impact of switching to observation alone might have counteracted any benefit or harm other management changes might have had on OS. In addition, cohorts 2 and 3 represent earlier timepoints in disease failure, and effects of changes in management from PSMA PET/CT may take longer patient follow-up to become evident.
Meanwhile, the pattern of disease spread, most specifically the mixed metastatic pattern, was an independent predictor of survival in all the cohorts included in the sub-analysis (HR 3.2, 7.6, and 2.8 for cohorts 2/3, 4, and 6, respectively). When looking more closely at the composition of this subgroup with worse OS, the vast majority of patients had a combination of lymph node and bone involvement (72.7%, 315/433). Karpinski et al. (10) developed two nomograms based on the PROMISE criteria to determine the risk of patients undergoing PSMA PET/CT for 3 and 5-year OS. In their nomogram predicting OS, the presence of extra-regional lymph nodes was the most significant factor to impact outcome, followed by burden of disease(10). In our analysis, the most significant factor predicting OS was the presence of mixed metastases, most of whom had a combination of lymph node and bone metastases. These differences may reflect differences in the definitions of the parameters chosen in each study. However, this should be further elucidated with future analyses of the study to determine if it is indeed the case. The reason behind this worse prognosis might be a more aggressive tumor biology, but it remains undetermined so far. Nevertheless, being able to identify groups where current therapeutic approaches are not enough will still be beneficial in the sense that it can allow us to explore different or more aggressive treatment alternatives that can positively impact their outcome.
What comes next?
Past and ongoing 18F-PSMA PET/CT studies continue to provide evidence that highlights the advantages of using this imaging modality in prostatic cancer patients. While in this study, its beneficial role in a subset of patients became evident, other cohorts need further follow-up or a larger sample size to be able to determine which role, if any, could PET/CT play in their follow-up and management. Furthermore, in this study, Gleason score/tumor grade was mostly available for cohorts that underwent RP and were, thus, younger, had shorter follow-up, and a lower number of events. These limitations prevented the study from having significant power in determining if a combination of PET/CT results and Gleason group could help further stratify patients into groups where more or less aggressive treatment could/should be pursued.
With the approval by Health Canada of two 68Ga-based tracers (i.e., Locametz and Illucix) and based on the data and analyses available through the PREP registry study, access to PSMA PET/CT in Ontario is now available as part of the routine standard of care (https://www.ontariohealth.ca/clinical/pet-scans). Analyses of the complete PREP population (estimated at about 10,000 men) accrued over the life of the Registry are planned and will provide additional real-world evidence about this innovation in prostate cancer management.
Written by:
- Andres Kohan, Department of Medical Imaging, University of Toronto, Toronto, Ontario, Canada
- Ur Metser, Department of Medical Imaging, University of Toronto, Toronto, Ontario, Canada
- Glenn Bauman, Department of Oncology, Western University, London, Ontario, Canada
- Schuster DM, Nanni C, Fanti S. PET Tracers Beyond FDG in Prostate Cancer. Semin Nucl Med. 2016; 46(6):507-21.
- Fraum TJ, Ludwig DR, Kim EH, Schroeder P, Hope TA, Ippolito JE. Prostate cancer PET tracers: essentials for the urologist. Can J Urol. 2018; 25(4):9371-83.
- Ma W, Mao J, Yang J, Wang T, Zhao ZH. Comparing the diagnostic performance of radiotracers in prostate cancer biochemical recurrence: a systematic review and meta-analysis. Eur Radiol. 2022; 32(11):7374-85.
- Dai YH, Chen PH, Lee DJ, Andrade G, Vallis KA. A Meta-Analysis and Meta-Regression of the Efficacy, Toxicity, and Quality of Life Outcomes Following Prostate-Specific Membrane Antigen Radioligand Therapy Utilising Lutetium-177 and Actinium-225 in Metastatic Prostate Cancer. Eur Urol. 2025; 87(4):398-408.
- Jani AB, Schreibmann E, Goyal S, et al. (18)F-fluciclovine-PET/CT imaging versus conventional imaging alone to guide postprostatectomy salvage radiotherapy for prostate cancer (EMPIRE-1): a single centre, open-label, phase 2/3 randomised controlled trial. Lancet. 2021; 397(10288):1895-904.
- Menard C, Young S, Zukotynski K, et al. PSMA PET/CT guided intensification of therapy in patients at risk of advanced prostate cancer (PATRON): a pragmatic phase III randomized controlled trial. BMC Cancer. 2022; 22(1):251.
- Kohan A, Metser U, Luke W, et al. A Prospective Provincial Registry of (18)F-PSMA PET/CT for Recurrent Prostate Cancer: Results for 4,135 Men. J Nucl Med. 2025; 66(8):1223-31.
- Metser U, Zukotynski K, Mak V, et al. Effect of (18)F-DCFPyL PET/CT on the Management of Patients with Recurrent Prostate Cancer: Results of a Prospective Multicenter Registry Trial. Radiology. 2022; 303(2):414-22.
- Tan VS, Metser U, Rashid M, et al. Association of marginalization and PSMA-PET in prostate cancer An analysis of the Ontario PSMA-PET Registry for Recurrent Prostate Cancer. Can Urol Assoc J. 2025; 19(6):193-201.
- Karpinski MJ, Husing J, Claassen K, et al. Combining PSMA-PET and PROMISE to re-define disease stage and risk in patients with prostate cancer: a multicentre retrospective study. Lancet Oncol. 2024; 25(9):1188-201.