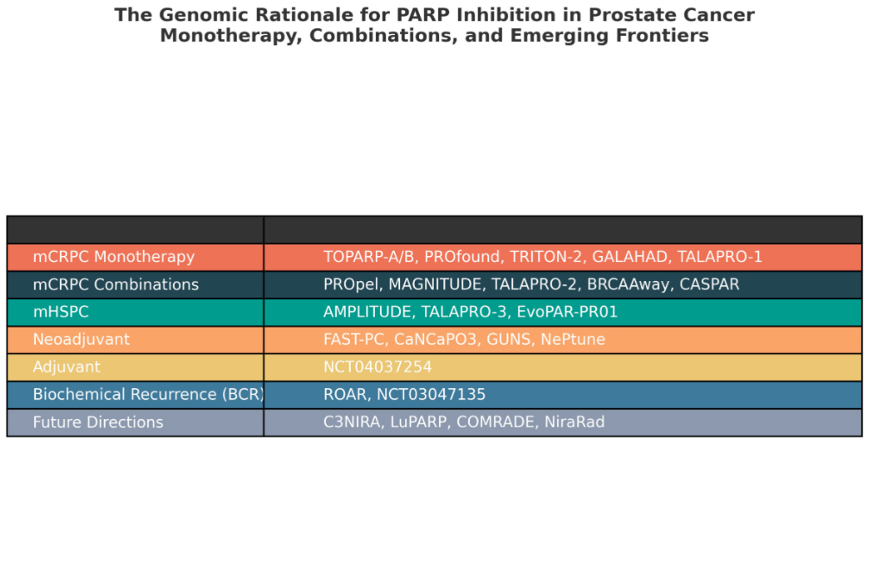
1. mCRPC Monotherapy
Early evidence from TOPARP-A/B showed that olaparib elicited responses in 88% of DDR-mutated tumors vs 6% in DDR–. The benefit was greatest in BRCA1/2 (median PFS 8.3 months), more modest in ATM (5.8 months), and limited in CDK12 (2.9 months).
Subsequent phase II (GALAHAD, TRITON-2, TALAPRO-1) and phase III studies (PROfound, TRITON-3) confirmed the gene-specific benefit:
- GALAHAD (Niraparib): ORR 34%, rPFS 8.1 months, and OS 13.0 months in BRCA, vs ORR 10%, rPFS 3.7 months, and OS 9.6 months in non-BRCA.
- TRITON-2 (Rucaparib): ORR 46%, PFS 10.7 months, and OS 17.2 months in BRCA, with remarkable efficacy in PALB2 (ORR 100%, rPFS 13.6 months), but negligible activity in ATM/CHEK2/CDK12.
- TALAPRO-1 (Talazoparib): ORR 46.2%, PFS 11.2 months in BRCA2, but only 6.7% and 3.5 months in ATM.
- PROfound (Olaparib): rPFS (7.4 vs 3.6 months; HR 0.34) and OS (19.1 vs 14.7 months; HR 0.69) in BRCA1/2 or ATM, with post-hoc analyses confirming the strongest benefit in BRCA1/2 (rPFS HR 0.22; OS HR 0.63).
- TRITON-3 (Rucaparib): In pre-chemotherapy mCRPC, rucaparib prolonged rPFS in BRCA1/2, but at ASCO-GU 2025 update, final OS did not reach significance (23.2 vs 21.2 months; HR 0.91). No benefit was seen in ATM (HR 1.21).
PARPi+ARPI combinations exploit AR–DDR crosstalk, inducing “BRCAness” in HRR-proficient tumors.
- PROpel (Olaparib+Abiraterone): rPFS 24.8 vs 16.6 months (HR 0.66) in ITT. BRCA1/2 derived the greatest benefit (HR 0.23). OS trended longer (42.1 vs 34.7 months, HR 0.81), significant in HRR+ (HR 0.66) and BRCA (HR 0.29).
- MAGNITUDE (Niraparib+Abiraterone): HRR– closed early. In HRR+, rPFS 16.7 vs 13.7 months (HR 0.76); in BRCA1/2, 19.5 vs 10.9 months (HR 0.55). OS not improved.
- TALAPRO-2 (Talazoparib+Enzalutamide): In the unselected all-comers population, rPFS was not reached versus 21.9 months (HR 0.63). Among patients with HRR+ tumors, rPFS was significantly prolonged at 30.7 months compared to 12.3 months (HR 0.47). Final overall survival (OS) data, presented at ASCO-GU 2025, demonstrated an 8.8-month improvement (45.1 vs 31.1 months; HR 0.62), establishing this regimen as a new standard of care for HRR+ mCRPC. At ASCO 2025, an exploratory gene subgroup analysis revealed pronounced benefit in BRCA2-mutated patients (ORR 86.4%, rPFS HR 0.25, OS HR 0.47), with additional gains observed in PALB2 and CDK12, and modest activity in CHEK2.
- BRCAAway (Abiraterone+Olaparib): phase II trial further emphasized the genomic rationale: in HRR-mutated mCRPC, abiraterone+olaparib yielded a median PFS of 39 months, compared with 14 months for olaparib and 8.4 months for abiraterone alone (HR 0.28 vs AAP; HR 0.32 vs olaparib).
- CASPAR (Enzalutamide+Rucaparib, ongoing): will clarify outcomes, including in non-BRCA disease.
Moving earlier in the disease, PARPi is under active investigation in metastatic hormone-sensitive prostate cancer (mHSPC).
- AMPLITUDE (Niraparib+abiraterone): The first interim analysis, reported at ASCO 2025, demonstrated a significant improvement with the combination in rPFS (NR vs 29.5 months; HR 0.63; p=0.0001), with an immature positive OS trend (HR 0.79). BRCA1/2 patients derived marked benefit (rPFS HR 0.52; OS HR 0.75).
- TALAPRO-3 (Talazoparib+enzalutamide): Talazoparib+enzalutamide vs enzalutamide in HRR-mutated mHSPC is ongoing
- EvoPAR-PR01 (Saruparib+hormonal therapy): under study in mHSPC regardless of HRR status.
4. New Frontiers
Neoadjuvant Setting
- FAST-PC (Fuzuloparib+Abiraterone): In high-risk localized PC, achieved 46% combined pCR/MRD and 53% 2-year bPFS, with faster PSA declines in BRCA2/HRR-mutated patients.
- CaNCaP03 (Olaparib±Degarelix): Showed PSA decline and PARP inhibition in pre-op samples.
- GUNS (Niraparib) & NePtune (Olaparib in BRCA1/2): evaluating pathologic response and MRD clearance.
- NCT04037254 (Niraparib+RT+ADT) reported a 30% PSA decline, rising to 33% in BRCA1/2. Adjuvant studies remain early-phase but promising.
- Biochemical Recurrence (BCR)
- ROAR (Rucaparib): PSA-PFS 35.3 months in high-risk HRR+ BCR, though the study closed early.
- NCT03047135 (Olaparib): HRR+ patients had PSA50 in 48%, including 100% of BRCA2.
- Combination strategies: PARPi with immunotherapy (C3NIRA: Niraparib+Cetrelimab improved OS 24.3 vs 10.2 months, p=0.01), or with radioligands (LuPARP, COMRADE, NiraRad).
- Functional biomarkers: Needed beyond genomics to stratify ATM/CDK12/CHEK2.
- Treatment sequencing: Determining optimal timing of monotherapy vs combination will be key to maximizing benefit and preventing resistance.
The benefit of PARP inhibition in prostate cancer is gene- and stage-specific.
- mCRPC monotherapy: Durable efficacy in BRCA1/2 and PALB2, limited in ATM, CHEK2, CDK12.
- mCRPC combinations: Extend survival across broader HRR+ populations, with TALAPRO-2 and PROpel confirming OS benefit, strongest in BRCA2.
- mHSPC (AMPLITUDE): Supports earlier use, especially in BRCA-driven disease.
- New frontiers (neoadjuvant, adjuvant, BCR): Open the door to PARPi in curative-intent settings, where HRR mutations may guide intensified therapy.
References:
Read the Abstract