The therapeutic landscape for metastatic castration-resistant prostate cancer (mCRPC) is evolving rapidly, and radioligand therapy may now serve as a cornerstone across all disease phases. From external beam radiotherapy in localised disease, to metastasis-directed therapy in the oligometastatic setting, and finally to Lutetium-based systemic treatments for advanced mCRPC, the radiation oncology armamentarium is becoming more integrated and comprehensive than ever before.
Our meta-analysis supports a potential paradigm shift: radioligand therapy should no longer be viewed solely as a late-line option but rather as a targeted and sustainable intervention that may be integrated earlier in the treatment pathway—particularly for patients with high disease burden or rapid PSA progression.
From a clinical perspective, [¹⁷⁷Lu]Lu-PSMA-617 provides a robust improvement in radiographic progression-free survival (rPFS), with the greatest relative advantage observed between 6 and 18 months. This window appears to be the optimal therapeutic phase, particularly for patients with aggressive disease characteristics. Interestingly, time-dependent survival analyses revealed that while the pooled hazard ratio for overall survival (HR = 0.81 [95% CI: 0.56–1.18]) did not reach statistical significance, a survival benefit becomes more apparent after 30 months, suggesting a delayed therapeutic effect that may be underappreciated in traditional HR-only meta-analyses.
To summarise the key clinical insights from this meta-analysis, the following table outlines the main outcomes:
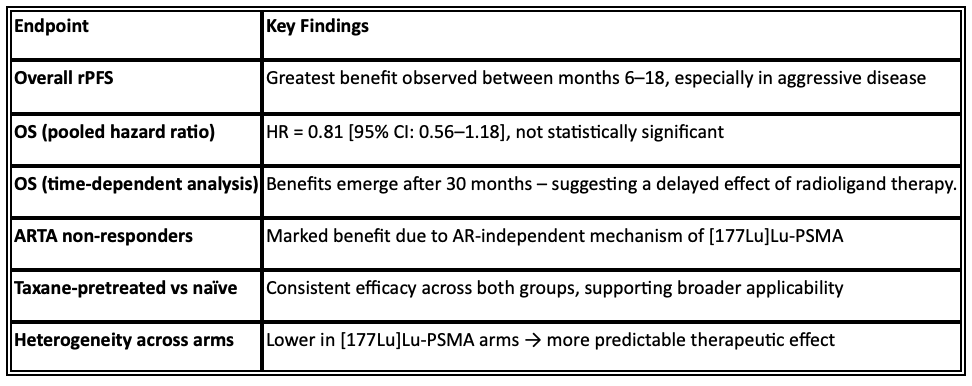
These subgroup findings reinforce the overall clinical narrative:
- Patients with high-volume disease and rapid PSA kinetics showed the most pronounced benefit from early radioligand therapy.
- Androgen Receptor-Targeted Agents (ARTA) non-responders particularly benefited, likely due to [¹⁷⁷Lu]Lu-PSMA’s AR-independent mechanism of action.
- Clinical outcomes were consistent regardless of prior taxane exposure, broadening the applicability of this therapy.
Economic Perspective: Break-Even Threshold Analysis
To evaluate the economic sustainability of [¹⁷⁷Lu]Lu-PSMA-617 compared with standard-of-care therapies, we conducted a Break-Even Cost Analysis based on a willingness-to-pay (WTP) threshold of €8,000 per additional month of radiographic progression-free survival (rPFS) gained.
We applied the following formula to determine the incremental cost per month of rPFS:

Where:
- CostLuPSMA is set at €120,000 (6 cycles × €20,000)
- CostSOC refers to either ARTA or Cabazitaxel, depending on the comparator
- rPFS is measured in months
In this scenario:
- rPFS for [¹⁷⁷Lu]Lu-PSMA = 14.6 months
- rPFS for ARTA = 12.1 months
- Incremental rPFS gain = 14.6 – 12.1 = 2.5 months

This means that [¹⁷⁷Lu]Lu-PSMA can cost up to €1,653 more per month than ARTA and still be considered cost-effective.
Alternatively, we can calculate the maximum monthly cost that ARTA could have while remaining competitive with [¹⁷⁷Lu]Lu-PSMA:

For ARTA to remain economically competitive, its monthly price should not exceed approximately €4,300–€4,400.
Comparison with Cabazitaxel
In this second scenario:
- rPFS for [¹⁷⁷Lu]Lu-PSMA = 14.6 months
- rPFS for Cabazitaxel = 11.3 months
- Incremental rPFS gain = 3.3 months
At a WTP of €8,000/month, the value of the incremental rPFS gain becomes:
This suggests that [¹⁷⁷Lu]Lu-PSMA may be considered cost-effective if its total cost is up to €26,400 higher than that of Cabazitaxel.
To derive the maximum monthly cost Cabazitaxel could sustain while remaining comparable:
Thus, Cabazitaxel would need to cost no more than ~€2,300 per month to remain economically viable in comparison to [¹⁷⁷Lu]Lu-PSMA.
Despite higher upfront costs, the fixed-cycle nature and early efficacy of [¹⁷⁷Lu]Lu-PSMA-617 make it a cost-effective option, particularly for patients with rapidly progressing disease. These break-even thresholds emphasise the importance of considering both clinical benefit and treatment duration when assessing economic value. Compared to continuously administered treatments like ARTA and Cabazitaxel, [¹⁷⁷Lu]Lu-PSMA demonstrates a favourable alignment with value-based oncology principles.
Break-Even Cost Analysis Table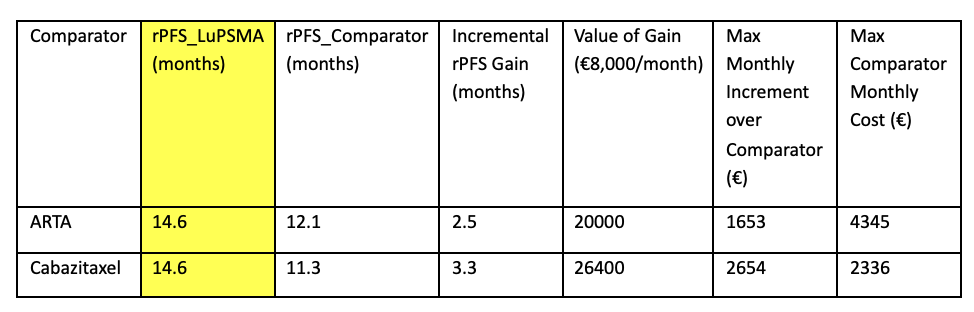
Written by: Francesco Fiorica, MD, PhD, Department of Clinical Oncology, Section of Radiation Oncology and Nuclear Medicine, Section of Medical Oncology, AULSS 9 Scaligera, Verona, Italy.
Read the Abstract