Several studies suggest that positron emission tomography/computed tomography (PET/CT) with different radiopharmaceuticals can impact oncological results. In particular, prostate-specific membrane antigen (PSMA) PET/CT has been associated with improvements in progression-free survival (PFS) and androgen deprivation therapy-free survival.4–8 Nevertheless, the robustness of these findings is limited by study heterogeneity and small sample sizes.
To address this, the PRECISE-MDT study included over 400 patients across eight Italian cancer centers.9
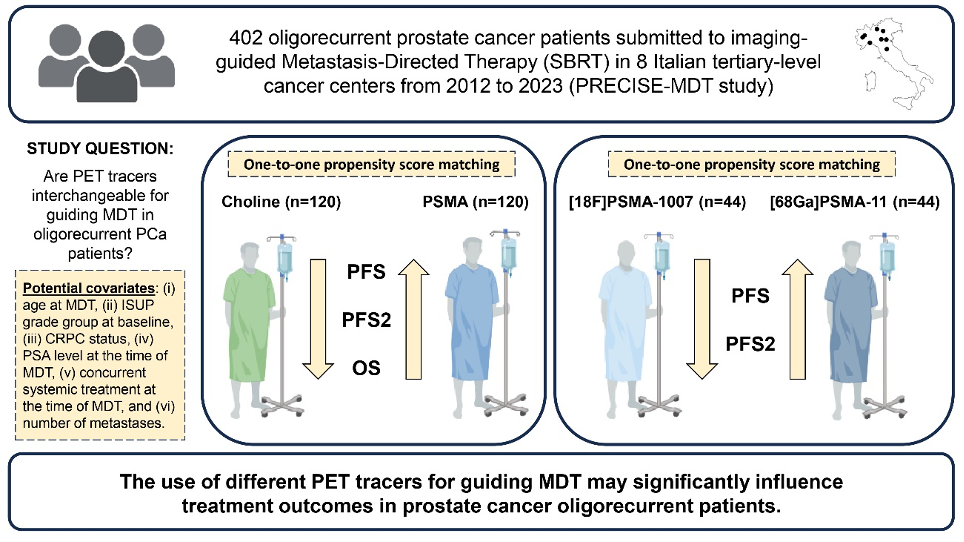
Figure 1. Design and main findings of the PRECISE-MDT study.9
The primary aim was to evaluate the association between the PET/CT modality used to guide MDT and long-term oncological outcomes. The endpoints assessed were PFS, PFS2 (time to systemic treatment change due to polymetastatic progression), and overall survival (OS). To minimize selection bias inherent to the retrospective design, both 1:1 propensity score matching and inverse probability of treatment weighting were applied. The study compared MDT guided by [18F]F-Fluorocholine, [68Ga]Ga-PSMA-11, and [18F]F-PSMA-1007 PET/CT.
In line with existing literature, PSMA PET/CT was associated with improved PFS and PFS2 compared to [18F]F-Fluorocholine PET/CT (p < 0.001 for both). Similarly, PSMA PET/CT guidance was linked to prolonged OS relative to [18F]F-Fluorocholine (p < 0.05). Moreover, [68Ga]Ga-PSMA-11 was associated with improved PFS (p < 0.05) and PFS2 (p < 0.005) compared with [18F]F-PSMA-1007.
To explore this further, we performed a secondary analysis focused on local and distant disease control in hormone-sensitive patients. 10 Restaging was conducted using the same imaging modality employed for the initial MDT. Among 241 patients (340 lesions), MDT guided by [68Ga]Ga-PSMA-11 PET/CT yielded superior metastasis-free survival (MFS not reached) compared with [18F]F-PSMA-1007 (median MFS 24.9 months; p < 0.001), which itself outperformed choline PET/CT (median MFS 18 months; p < 0.001). These findings extend across both nodal and bone metastases (p < 0.001 for both).
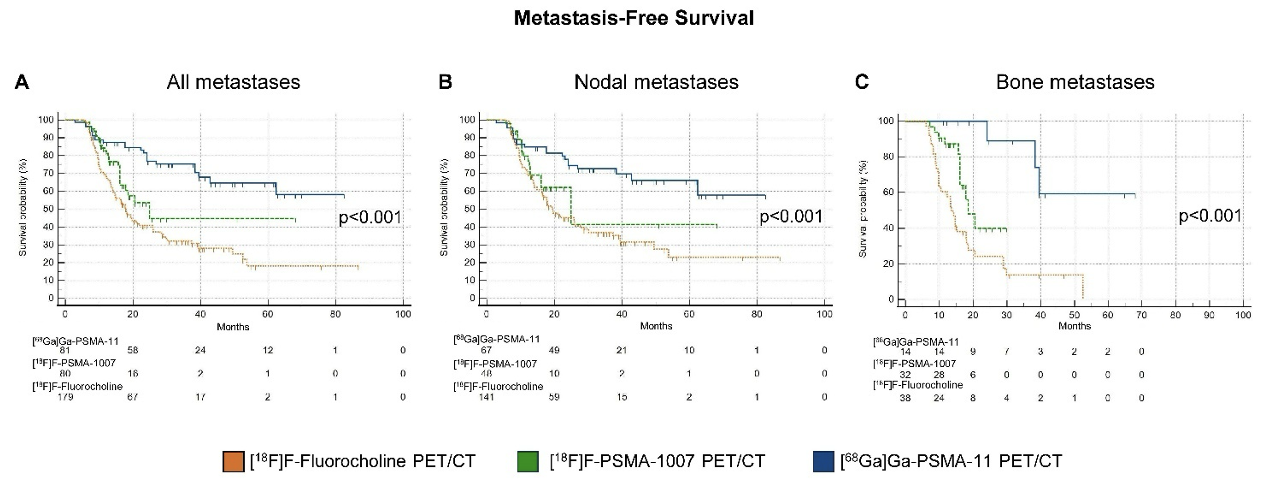
Figure 2. Kaplan-Meier curves for MFS according to the PET/CT radiopharmaceutical used to guide MDT in (A) all lesions, (B) nodal, and (C) bone metastases.
In contrast, no significant differences in local disease control were observed across the three PET/CT modalities (median local recurrence-free survival, LRFS, not reached for all; p = 0.73 for all lesions, p = 0.52 for nodal metastases, and p = 0.69 for bone metastases).

Figure 3. Local and distant disease control rates according to the PET/CT radiopharmaceutical used to guide MDT in oligorecurrent hormone-sensitive PCa patients from the PRECISE-MDT cohort.
The lack of differences in local disease control aligns with existing evidence: choline PET/CT has demonstrated good specificity for PCa lesion identification, but lower sensitivity and detection rates compared with [68Ga]Ga-PSMA-11 and [18F]F-PSMA-1007, particularly at low PSA levels. This likely explains the superior MFS achieved with PSMA-guided MDT, emphasizing the importance of sensitive imaging modalities for improved distant disease control.
It is important to interpret these findings in light of the retrospective design and potential confounding from systemic treatments. Advances in systemic therapy for PCa have significantly improved outcomes in the oligometastatic hormone-sensitive setting. To account for this, we performed supplementary analyses excluding patients who received concurrent systemic therapy.11 Even in this subgroup, PSMA PET/CT-guided MDT remained independently associated with improved PFS (p < 0.001) and PFS2 (p = 0.005) compared with choline PET/CT, reinforcing the robustness of the results.
The optimal PSMA ligand for clinical practice, however, remains uncertain. Notably, [18F]F-PSMA-1007 demonstrates higher uptake in benign nodal and bone lesions—termed unspecific bone uptake (UBU)—compared with [68Ga]Ga-PSMA-11.12 This complicates interpretation, especially for less experienced readers.13,14 True bone metastases may be misclassified as UBU, potentially leading to undertreatment, while nonspecific uptake during follow-up might be misinterpreted as recurrence, resulting in premature systemic therapy changes. These issues may partly explain the superior MFS associated with [68Ga]Ga-PSMA-11. Importantly, since no central scan review was conducted, our findings may reflect real-world practice, where physicians of varying expertise face the challenges of interpreting [18F]F-PSMA-1007 PET/CT images.
Take-home messages:
- MDT guided by [68Ga]Ga-PSMA-11 outperformed [18F]F-PSMA-1007 and [18F]F-Fluorocholine, delivering superior distant disease control.
- The advantage of [68Ga]Ga-PSMA-11 extends across both nodal and bone metastases.
- Prospective trials are needed to confirm these results and define the best imaging strategy for personalized MDT.
Written by: Matteo Bauckneht, MD, PhD, and Francesco Lanfranchi, MD
Nuclear Medicine Unit, University of Genova and IRCCS Ospedale Policlinico San Martino, Genova, Italy.
References:
- Ost P, Reynders D, Decaestecker K, et al. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J Clin Oncol. 2018;36(5):446-453. doi:10.1200/JCO.2017.75.4853
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol. 2020;6(5):650-659. doi:10.1001/jamaoncol.2020.0147
- Deek MP, Van der Eecken K, Sutera P, et al. Long-Term Outcomes and Genetic Predictors of Response to Metastasis-Directed Therapy Versus Observation in Oligometastatic Prostate Cancer: Analysis of STOMP and ORIOLE Trials. J Clin Oncol. 2022;40(29):3377-3382. doi:10.1200/JCO.22.00644
- Schmidt Hegemann NS, Rogowski P, Eze C, et al. Outcome After 68Ga-PSMA-11 versus Choline PET-Based Salvage Radiotherapy in Patients with Biochemical Recurrence of Prostate Cancer: A Matched-Pair Analysis. Cancers (Basel). 2020;12(11):3395. Published 2020 Nov 16. doi:10.3390/cancers12113395
- Deijen CL, Vrijenhoek GL, Schaake EE, et al. PSMA-11-PET/CT versus choline-PET/CT to guide stereotactic ablative radiotherapy for androgen deprivation therapy deferral in patients with oligometastatic prostate cancer. Clin Transl Radiat Oncol. 2021;30:1-6. Published 2021 Jun 29. doi:10.1016/j.ctro.2021.06.004
- Mazzola R, Francolini G, Triggiani L, et al. Metastasis-directed Therapy (SBRT) Guided by PET-CT 18F-CHOLINE Versus PET-CT 68Ga-PSMA in Castration-sensitive Oligorecurrent Prostate Cancer: A Comparative Analysis of Effectiveness. Clin Genitourin Cancer. 2021;19(3):230-236. doi:10.1016/j.clgc.2020.08.002
- Lanfranchi F, Belgioia L, Marcenaro M, et al. Oligometastatic Prostate Cancer Treated with Metastasis-Directed Therapy Guided by Positron Emission Tomography: Does the Tracer Matter?. Cancers (Basel). 2023;15(1):323. Published 2023 Jan 3. doi:10.3390/cancers15010323
- Metz R, Rauscher A, Vaugier L, et al. Comparison of Hormone-Sensitive Oligorecurrent Prostate Cancer Patients Based on Routine Use of Choline and/or PSMA PET/CT to Guide Metastasis-Directed Therapy. Cancers (Basel). 2023;15(6):1898. Published 2023 Mar 22. doi:10.3390/cancers15061898
- Bauckneht M, Lanfranchi F, Albano D, et al. Diverse Imaging Methods May Influence Long-Term Oncologic Outcomes in Oligorecurrent Prostate Cancer Patients Treated with Metastasis-Directed Therapy (the PRECISE-MDT Study). J Nucl Med. 2024;65(8):1202-1209. Published 2024 Aug 1. doi:10.2967/jnumed.124.267586
- Lanfranchi F, Belgioia L, Albano D, et al. Impact of Metastasis-directed Therapy Guided by Different PET/CT Radiotracers on Distant and Local Disease Control in Oligorecurrent Hormone-sensitive Prostate Cancer: A Secondary Analysis of the PRECISE-MDT Study. Radiol Imaging Cancer. 2025;7(3):e240150. doi:10.1148/rycan.240150
- Bauckneht M, Lanfranchi F, Belgioia L. Reply: One Bite from the Apple, One Bite from the Orange in the PRECISE-MDT Study and Limitations of Retrospective Study Design and Potential Bias in the PRECISE-MDT Study. J Nucl Med. 2024;65(12):1986. Published 2024 Dec 3. doi:10.2967/jnumed.124.268781
- Rizzo A, Morbelli S, Albano D, et al. The Homunculus of unspecific bone uptakes associated with PSMA-targeted tracers: a systematic review-based definition. Eur J Nucl Med Mol Imaging. 2024;51(12):3753-3764. doi:10.1007/s00259-024-06797-5
- Bauckneht M, D'Amico F, Albano D, et al. Composite Prediction Score to Interpret Bone Focal Uptake in Hormone-Sensitive Prostate Cancer Patients Imaged with [18F]PSMA-1007 PET/CT. J Nucl Med. 2024;65(10):1577-1583. Published 2024 Oct 1. doi:10.2967/jnumed.124.267751
- Bauckneht M, Pasini G, Di Raimondo T, et al. [18F]PSMA-1007 PET/CT-based radiomics may help enhance the interpretation of bone focal uptakes in hormone-sensitive prostate cancer patients. Eur J Nucl Med Mol Imaging. 2025;52(6):2076-2086. doi:10.1007/s00259-025-07085-6