Conventional computed tomography and ultrasound, while useful for guiding diagnostic and therapeutic interventions on a whole prostate level, are limited in delineating the extent of intra-prostatic disease. Magnetic resonance imaging and positron emission tomography using prostate cancer targeting radiopharmaceuticals (i.e. PSMA) allow the detection and delineation of intra-prostatic foci (IPF) with good to excellent performance (AUC 0.8 or better – Dhar review). Delineation of such intra-prostatic foci enables more accurate tissue sampling through targeted biopsy (PRECISE, PRECISION studies) and optimized therapies through tissue sparing (i.e. focal therapy) or focal intensification (i.e. microboosts).
The FLAME phase III trial demonstrated improved clinical outcomes (BF and MFS) among men with dose escalation (up to 90Gy) using multiparametric MR for delineation of IPF for “micro-boosting”. Importantly, such dose escalation was limited by organ at risk (OAR) constraints; thus, the median D98 IPF boost dose was 84.7 Gy with a median boost volume of 2.9cm3.1 Secondary analyses demonstrated a clear dose response in terms of local control with increased microboost dosing. Capitalizing on the increasing use of ultra-hypofractionation, the Phase II HYPOFLAME trial demonstrated the safety of using MR guided microboosting with a whole prostate dose of 35Gy/5 fractions with microboost doses up to 50Gy/5 fractions.2
While multiparametric MRI can demonstrate intra-prostatic foci and the PiRADs guidelines codify the interpretation of these images, mpMRI is still subject to some limitations. For example, even in the use of PiRADs criteria, significant reader variability and IPF delineation can still exist. Furthermore, MRI to histology correlations suggest MRI may underestimate actual tumor volumes, and some cancers may be “invisible” on MRI. More recently, PSMA targeting PET imaging has demonstrated excellent performance in delineating IPF, tends to track more closely with actual IPF tumor volumes, and may be more straightforward to standardize in terms of IPF delineation through SUV windowing and thresholding guidelines. In studies comparing MRI and PSMA PET, both studies are complementary, with improved performance with combined PET/MRI compared to either modality alone.
While FLAME and HYPOFLAME (and other studies) have demonstrated the efficacy and safety of MRI based microboosting, there are fewer studies examining these questions using PSMA PET based radiation planning and delivery. Recently, Zambuglou et al.3 reported on a Phase II trial (HypoFocal ARO2020-01) demonstrating the safety of PSMA PET and MRI based micro boosting using either external beam or brachytherapy and have launched the Phase III trial HypoFocal-SBRT.4
Another gap in our information is the evolution of IPF imaging after treatment. While it is known through serial post-treatment biopsy studies that it may take up to three years for complete histologic clearance of cancer from the prostate, there is a dearth of prospective studies with serial imaging to characterize longitudinal imaging changes in treated prostate cancer foci. Available studies suggest that MRI changes may track with histological findings, with the resolution of MRI detected IPF taking years to resolve. The limited information available for PSMA PET suggests that changes in PSMA SUV may pick up earlier response, with maximum SUV response noted between 6-12 months in the available series.
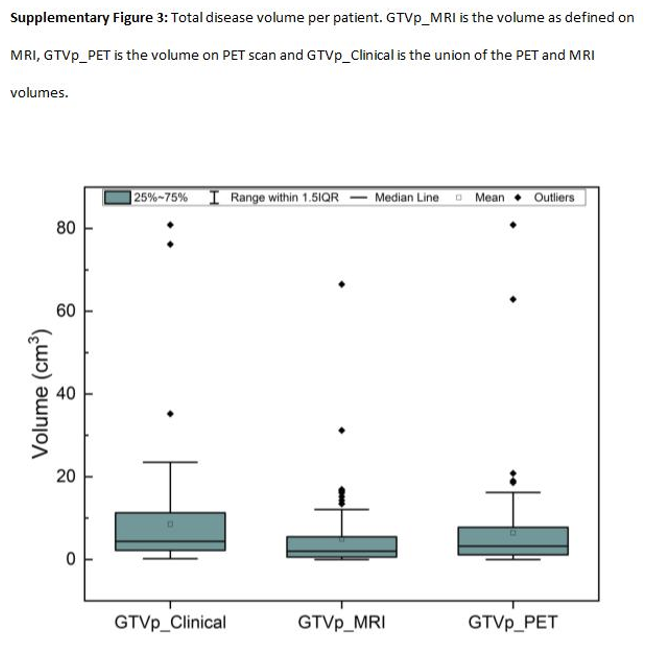
It is on this background that the ARGOS/CLIMBER study was initiated to explore both the safety as well as the long-term response to ultra-hypofractionated stereotactic radiotherapy with micro-boost for men with high intermediate to high-risk prostate cancer. Like HYPOFLAME, a whole prostate dose of 35Gy/5 fractions given every other day was used, and a micro-boost up to 50Gy/5 was allowed, but IPF was delineated as the union of gross tumor volumes (GTV) delineated on both MRI and [18F]-1007 PSMA PET imaging. The institutional availability of hybrid PET/MRI was exploited for this trial and the two participating sites, but the treatment workflow could also be reproduced with separate mpMRI and PET/CT studies. Pre-treatment imaging was fused with standard CT scans for radiation planning, with particular attention to bowel preparation (daily fleet enemas prior to planning and treatment visits) and a standardized bladder filling protocol. All men had implanted fiducials, and these were placed after the acquisition of the baseline PET/MRI to avoid the introduction of imaging artifacts from the fiducials. Meticulous attention was paid to OAR delineation, particularly to the intra-prostatic urethra (where MRI and retrograde urethrogram at the time of CT simulation aided in delineation). Micro boost dose per patient varied according to OAR constraints, and we found that the limiting structure in most cases was the intra-prostatic urethra. Ultimately, a median prostate micro boost of 41.6 Gy (IQR: 39.3-44.8 Gy) was delivered to a median of 1 intra-prostatic lesion. In delineating lesions on PET we used the criteria recommended by Zamboglou, with thresholding according to an SUVmax of 20-40% depending on the uptake (less conspicuous lesions required a higher threshold value). We found that across our cases, GTVs delineated on MR were generally smaller than those delineated with PET, and the treated micro boost volume correlated more with the overall PET volume (Figure). IPF was present in 49/50 men, with a total of 84 IPF identified for boosting. Of the 84, 10 were visible on MR only and 6 on PET only. The remainder of lesions had overlap between the PET and MRI identified IPF. The median boost volume (union of MRI and PET) was 4.4 cm3, similar to that noted by Zamboglou in their trial (median 3.8cm3 for union of PET and MRI IPF) but larger than those noted on FLAME (2.9cm3, MR only). Following radiotherapy, all men went on to adjuvant ADT for 6-18 months (depending on risk category) after radiotherapy; neoadjuvant ADT was not performed to avoid confounding IPF detection and delineation on the baseline PET/MRI.
The primary endpoint of the trial (ARGOS component) was safety, and we saw a low rate of acute and intermediate GI and GU toxicity. Our single case of Grade 4 late GI toxicity was a man with initially Grade 1 rectal bleeding who was investigated by colonscopy at that time and was treated with APC and developed a fistula post APC. Thus, while the toxicity is attributed to radiotherapy, a more conservative approach to the rectal bleeding would have resulted in a lower grade of late GI toxicity.
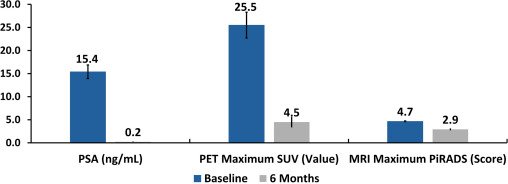
The CLIMBER component of the study includes comprehensive tissue and liquid biospecimen analysis. We are conducting detailed genomic and spatial proteinomic analysis of pre-treatment biopsies, along with analysis of urine and blood specimens. CLIMBER also includes longitudinal biospecimen and imaging acquisition, including PSMA PET/MRI at 6 months post treatment and at 24 months post treatment. Men are strongly encouraged (but not required) to undergo confirmatory transperineal prostate biopsy at 24 months for correlation with post treatment imaging. We will examine histologic clearance of prostate cancer at 24 months as well as changes in genomic and proteinomic profiles compared to baseline. To date, 48/50 men have had 6-month post treatment PSMA PET/MRI imaging (two patients had early relapse and were not imaged). At 6 months, median SUVmax declined from 25.5 to 4.5, with 21 (44.7%) men demonstrating a complete response (SUVmax in prostate decline to background) and 23 (48.9%) demonstrating a partial response. Median PiRADs scored declined from 4.7 to 2.9. Median PSA levels declined from 15 to 0.18 ng/ml. Correlation of these early biomarker responses with longer term endpoints (24 month biopsy and 60 month disease free survival) will help us determine if these early responses track with longer term cancer control.
Given the challenges we faced in escalating IPF due to OAR dose limitations, we have since opened an expansion study examining the integration of neoadjuvant hormone therapy with the ARGOS/CLIMBER workflow. In the expansion study, PSMA PET/MRI is obtained prior to any therapy and after three months of ADT as a baseline prior to radiotherapy, with total ADT duration remaining 6-18 months, depending on risk categorization. A follow-up PSMA PET/MRI is obtained at 6 months post radiotherapy. This expansion cohort has been fully subscribed, and we’ve noted that three months of neoadjuvant hormone therapy has been associated with smaller GTV volumes compared to the original ARGOS cohort and has facilitated micro boosting to higher median values. We also noted less conspicuity of PSMA avid foci with the use of neoadjuvant ADT, and as a consequence, thresholding for IPF delineation tended to be higher (40-60% SUV max). Future work will include looking at PET and MR response to neoadjuvant alone and 6 months post treatment, and comparing to the original ARGOS cohort, as well as looking at five year disease free survival between the two cohorts.
ARGOS/CLIMBER adds to the collective experience within our health care system using ultra-hypofractionated treatments for intermediate and high risk prostate cancer and aligns with the safety noted in other studies with longer term follow-up. [Ref] While stereotactic radiotherapy with or without micro boost represents one strategy for dose escalated radiotherapy, the combination of brachytherapy and external beam radiotherapy is another strategy demonstrated to be safe and efficacious (ASCENDE-RT). An international study, ASCENDE-SBRT will compare these strategies directly and is now open for accrual. The provision of micro boost is allowed in this study, and future sub-analyses looking at micro boosting within the context of this study could provide additional information as to the benefit of incorporating advanced imaging into dose escalated precision radiotherapy.Written by: Glenn Bauman, MD, FRCPC, Department of Oncology, Division of Radiation Oncology, London Health Sciences Centre and Western University, London, Ontario, Canada
References:
- Monninkhof EM., van Loon JWL., van Vulpen M. et al. Standard whole prostate gland radiotherapy with and without lesion boost in prostate cancer: Toxicity in the FLAME randomized controlled trial. Radiotherapy and Oncology. 2018. doi.org/10.1016/j.radonc.2017.12.022.
- De Cock L., Draulans C., Pos FJ. et al. From once-weekly to semi-weekly whole prostate gland stereotactic radiotherapy with focal boosting: primary endpoint analysis of the multicenter phase II hypo-FLAME 2.0 trial. Radiother Oncol. 2023 Aug:185:109713. doi: 10.1016/j.radonc.2023.109713.
- Zamboglou C., Spohn SKB., Ruf J. et al. PSMA-PET- and MRI-Based Focal Dose Escalated Radiation Therapy of Primary Prostate Cancer: Planned Safety Analysis of a Nonrandomized 2-Armed Phase 2 Trial (ARO2020-01). International Journal of Radiation Oncology, Biology, Physics. 2025. doi.org/10.1016/j.ijrobp.2022.04.020.
- Zamboglou C., Spohn SKB., Adebahr S. et al. PSMA-PET/MRI-Based Focal Dose Escalation in Patients with Primary Prostate Cancer Treated with Stereotactic Body Radiation Therapy (HypoFocal-SBRT): Study Protocol of a Randomized, Multicentric Phase III Trial. Cancers (Basel). 2021 Nov 18;13(22):5795. doi: 10.3390/cancers13225795.