With an estimated 299,010 new cases in 2024, prostate cancer is the most common cancer affecting men in the United States (Figure 1).1 In fact, prostate cancer alone accounts for 29% of incident cancer cases in men and 14.9% of all incident cancer cases.1 Interestingly, the five-year relative survival rate of localized prostate cancer has been estimated to be greater than 99%.2
Despite this favorable survival estimate for localized diseases, prostate cancer is still predicted to contribute to 35,250 new cancer deaths in 2024.1 This accounts for 5.8% of all cancer-driven deaths in the United States, rendering prostate cancer as the second leading cause of cancer-driven deaths in men1,2 (Figure 1). This suggests that the main driver behind prostate cancer mortality comes from the progression into metastatic diseases.3,4 In fact, as the cancer progresses into distant metastasis, the five-year relative survival rate drastically decreases from the >99% seen in localized and regional prostate cancers to a mere 30.2% in metastatic prostate cancer.2,3 Therefore, it is important to identify targets that drive prostate cancer’s progression toward metastasis and identify ways to predict metastatic onset.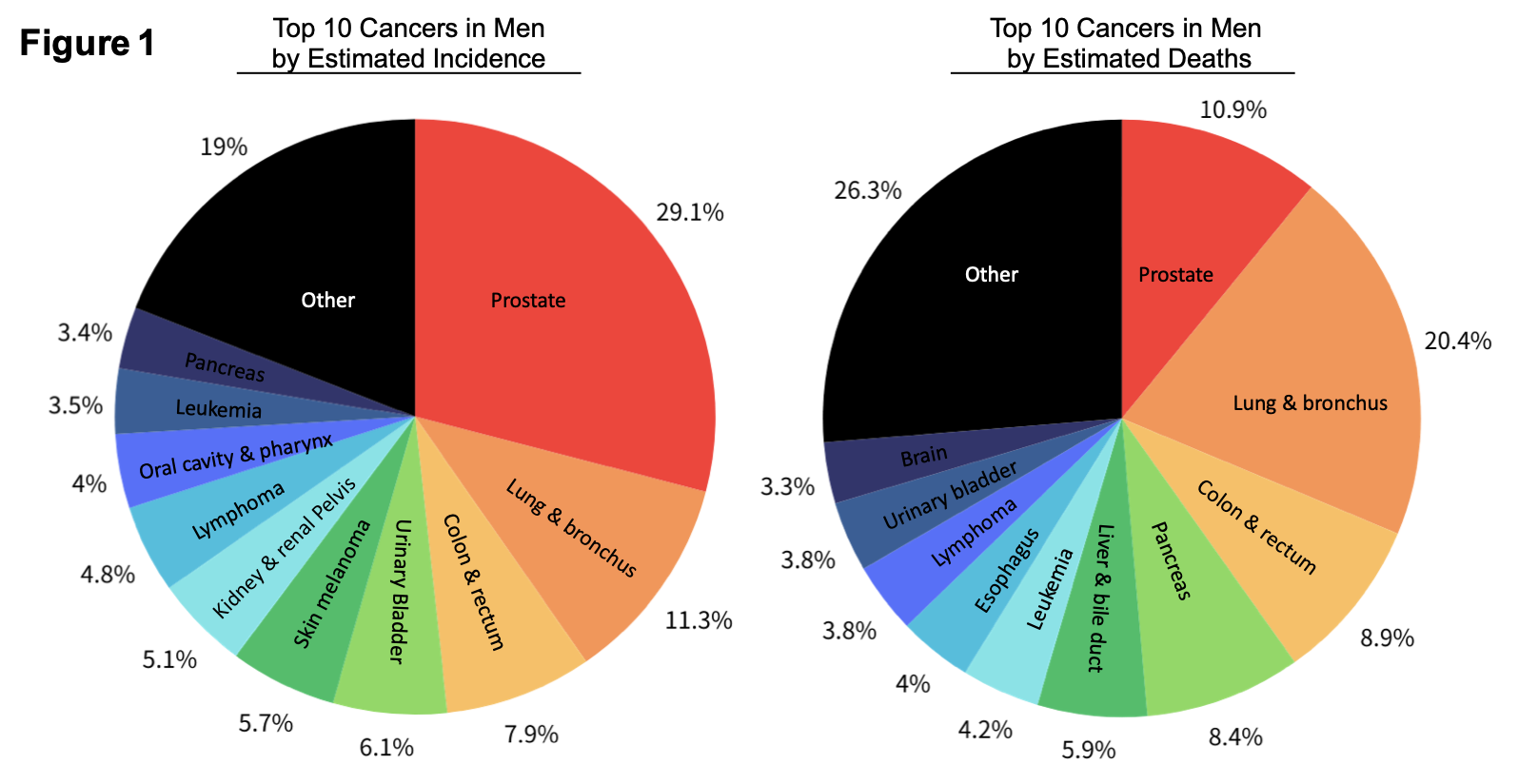
Figure 1. Top 10 Cancer Origins Affecting United States Men by Estimated 2024 Incidence and by Estimated 2024 Deaths. Incidence and death estimates were obtained from Cancer Statistics, 2024. The percentages of each of the top 10 cancers are labeled next to the corresponding pie. Pie charts generated via Canva.com.
Currently, prostate cancer risks are assessed using factors like prostate-specific antigen (PSA) levels, Gleason score, and the extent of tumor spread (staging).9 However, Gleason score and staging cannot be assessed continuously since they require biopsies, digital rectal exams, and/or surgery. PSA levels can be monitored more regularly since it is a minimally invasive test. However, elevated PSA levels can lead to false positives since an increase in PSA levels is not specific to prostate cancer and can also be caused by conditions such as old age, benign prostate hyperplasia, prostatitis, and urinary tract infections.10,11 This lack of cancer specificity and age-related variables makes it challenging to use standalone PSA levels in prognosis and metastasis prediction.12,13 While imaging techniques have improved the ability to detect clinically significant prostate cancer and reduced the number of unnecessary biopsies, new molecular methods to predict prostate cancer progression and metastasis are still needed.14 Genetic and transcriptomic markers have been proposed to monitor treatment effectiveness, predict the likelihood of treatment resistance and or recurrence, and stratify patients based on disease prognosis.15 For instance, Prostate Cancer Antigen 3 (PCA3), and SelectMDx are both urine-based mRNA tests to improve diagnostic accuracy of clinically significant prostate cancer with a higher specificity than PSA levels.16,17 However, the clinical space still needs a tool to predict the onset of prostate cancer metastasis, which is a critical contributor to prostate cancer-driven mortality. We also lack curative treatment strategies for these patients whose cancers have advanced into metastasis.18 Therefore, the potential to reduce prostate cancer-driven mortality lies in early risk assessment of prostate cancer progression, timely treatment to prevent metastatic onset, and the development of new treatments for metastatic diseases.
To generate a new approach to predict prostate cancer progression towards metastasis, this study utilized proteomic profiling and rapid autopsy samples from localized and metastatic prostate cancer patients to identify molecular indicators that are associated with prostate cancer metastasis (Figure 2). We first searched for protein candidates that are positively associated with prostate cancer metastasis through proteomic profiling, which identified 154 upregulated proteins that are positively associated with prostate cancer metastasis. We further screened these protein candidates in multiple independent patient datasets to assess the clinical applications of their mRNA expressions. Candidates that made it to our final 5-gene panel all have mRNA expressions that positively correlate with poor prognostic variables associated with prostate cancer progression, including biochemical recurrence, worse disease-free survival, and metastasis (Figure 2). The combined 5-gene panel also has an improved ability to predict metastasis relative to individual candidates in two additional independent datasets. In addition to prognosis prediction, the protein candidates discovered via proteomics can be further analyzed to assess the functional role they exert towards the progression into metastatic prostate cancer. Since we still lack effective treatment strategies for metastatic prostate cancer, these protein candidates can be assessed in further studies to determine their therapeutic potential as targets for metastatic prostate cancer.
By presenting new molecular indicators associated with prostate cancer metastasis on both protein and mRNA levels, we hope to contribute to the development of novel prognostic prediction and treatment tools to help physicians and patients overcome this prevalent disease.
Figure 2

Figure 2. Screening Schematic to Search for Molecular Indicators of Prostate Cancer Metastasis. Localized and metastatic patient samples were obtained from the prostate cancer rapid autopsy program. Proteomic profiling was performed to find candidates with elevated protein expression in metastasis relative to localized samples. These candidates were then screened in additional independent patient datasets to assess the ability of their mRNA expressions to predict clinical prognosis associated with prostate cancer progression, including biochemical recurrence, worse disease-free survival, and a positive association with metastatic onset. The candidates who passed these screenings have the potential to differentiate patients with a higher risk of metastasis.
Written by: Michelle Shen1 and Tanya Stoyanova, PhD1,2
- Department of Molecular and Medical Pharmacology, University of California, Los Angeles, Los Angeles, CA, USA
- Department of Urology, University of California, Los Angeles, Los Angeles, CA, USA
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74(1):12-49.
- Zhang AC, Rasul R, Golden A, Feuerstein MA. Incidence and mortality trends of metastatic prostate cancer: Surveillance, Epidemiology, and End Results database analysis. Can Urol Assoc J. 2021;15(12): E637-E43.
- Stoletov K, Bond D, Hebron K, Raha S, Zijlstra A, Lewis JD. Metastasis as a therapeutic target in prostate cancer: a conceptual framework. Am J Clin Exp Urol. 2014;2(1):45-56.
- Fares J, Fares MY, Khachfe HH, Salhab HA, Fares Y. Molecular principles of metastasis: a hallmark of cancer revisited. Signal Transduct Target Ther. 2020;5(1):28.
- (IQWiG) IfQaEiHC. Localized prostate cancer: Learn More – Low-risk prostate cancer: Active surveillance or treatment? 2022.
- Soloway MS, Soloway CT, Eldefrawy A, Acosta K, Kava B, Manoharan M. Careful selection and close monitoring of low-risk prostate cancer patients on active surveillance minimizes the need for treatment. Eur Urol. 2010;58(6):831-5.
- Society AC. Initial Treatment of Prostate Cancer, by Stage and Risk Group: Atlanta: American Cancer Society; 2022 [updated August 9, 2022.
- Burgess L, Roy S, Morgan S, Malone S. A Review on the Current Treatment Paradigm in High-Risk Prostate Cancer. Cancers (Basel). 2021;13(17).
- Eastham JA AG, Barocas DA, et al. Clinically localized prostate cancer: AUA/ASTRO guideline, part I: introduction, risk assessment, staging, and risk-based management. J Urol. 2022;208(1):10-18.
- Lumbreras B, Parker LA, Caballero-Romeu JP, Gomez-Perez L, Puig-Garcia M, Lopez-Garrigos M, et al. Variables Associated with False-Positive PSA Results: A Cohort Study with Real-World Data. Cancers (Basel). 2022;15(1).
- Nadler RB, Humphrey PA, Smith DS, Catalona WJ, Ratliff TL. Effect of inflammation and benign prostatic hyperplasia on elevated serum prostate specific antigen levels. J Urol. 1995;154(2 Pt 1):407-13.
- Thomsen FB, Westerberg M, Garmo H, Robinson D, Holmberg L, Ulmert HD, et al. Prediction of metastatic prostate cancer by prostate-specific antigen in combination with T stage and Gleason Grade: Nationwide, population-based register study. PLoS One. 2020;15(1):e0228447.
- Adamy A, Yee DS, Matsushita K, Maschino A, Cronin A, Vickers A, et al. Role of prostate specific antigen and immediate confirmatory biopsy in predicting progression during active surveillance for low risk prostate cancer. J Urol. 2011;185(2):477-82.
- Haj-Mirzaian A, Burk KS, Lacson R, Glazer DI, Saini S, Kibel AS, et al. Magnetic Resonance Imaging, Clinical, and Biopsy Findings in Suspected Prostate Cancer: A Systematic Review and Meta-Analysis. JAMA Netw Open. 2024;7(3):e244258.
- Alarcon-Zendejas AP, Scavuzzo A, Jimenez-Rios MA, Alvarez-Gomez RM, Montiel-Manriquez R, Castro-Hernandez C, et al. The promising role of new molecular biomarkers in prostate cancer: from coding and non-coding genes to artificial intelligence approaches. Prostate Cancer Prostatic Dis. 2022;25(3):431-43.
- Bourdoumis A, Papatsoris AG, Chrisofos M, Efstathiou E, Skolarikos A, Deliveliotis C. The novel prostate cancer antigen 3 (PCA3) biomarker. Int Braz J Urol. 2010;36(6):665-8; discussion 9.
- Hendriks RJ, van der Leest MMG, Israel B, Hannink G, YantiSetiasti A, Cornel EB, et al. Clinical use of the SelectMDx urinary-biomarker test with or without mpMRI in prostate cancer diagnosis: a prospective, multicenter study in biopsy-naive men. Prostate Cancer Prostatic Dis. 2021;24(4):1110-9.
- Yamada Y, Beltran H. The treatment landscape of metastatic prostate cancer. Cancer Lett. 2021;519:20-9.