An important discovery from the combined analysis was that patients with a high-risk mutational signature (defined by somatic mutations in ATM, BRCA1/2, Rb1, or TP53) had worse PFS of 7.5 months as opposed to 13.4 months in patients without a mutation. From these studies, we have gained insights that not all oligometastatic patients benefit from SBRT in equal magnitude regarding clinical outcomes and genomic alterations can play an important role in post-SBRT outcomes. A major finding of these past studies is that a subset of patients (±15-20%) with omCSPC demonstrate durable disease-free survival from SBRT alone, thereby delaying or avoiding the use of systemic therapy. Even with the use of highly sensitive molecular imaging modalities (e.g. PSMA-PET/CT), identifying these long-term responders to SBRT remains an important unmet need.
In a recent study published in Clinical Cancer Research,4 Andrews JR et al investigated the utility of PSMA-expressing extracellular vesicles (PSMA+ EVs) to risk-stratify patients with omCSPC. Extracellular vesicles (EVs) are microscopic particles released by benign and malignant cells into biofluids such as blood and urine. They carry molecular cargo (DNA, RNA, proteins) and surface antigens from donor cells, offering opportunities for the development of non-invasive biomarkers. Dr. Fabrice Lucien and his team previously demonstrated that circulating levels of PSMA+ EVs correlate with tumor burden in prostate cancer.5 In a multi-institutional collaboration, Andrews JR et al analyzed the levels of PSMA+ EVs in pre-SBRT plasma samples obtained from ORIOLE and STOMP-like cohorts and showed that patients with low levels of PSMA+ EVs have longer PFS compared to those with elevated concentrations (Figure 1).
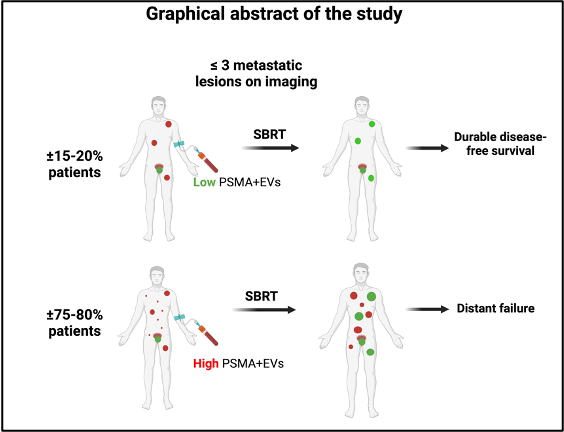
With a median follow-up of 45.7 months, median biochemical PFS was 26.1 vs. 15.0 months (p=0.005), and median radiographical PFS was 36.0 vs. 25.0 months (p=0.003) for PSMA+EV low vs. high groups, respectively. Importantly, PSMA+ EVs also served as predictive biomarkers. In the ORIOLE cohort, omCSPC patients with low PSMA+ EVs benefited from SBRT when compared to observation (median biochemical PFS of 24.3 vs. 5.8 months; p=0.003) whereas no benefit with SBRT was noted in patients with high PSMA+ EVs (median biochemical PFS of 5.9 vs 7.1 months; p=0.95). Based on this, patients with elevated PSMA+ EVs might benefit from systemic therapy escalation in addition to SBRT.
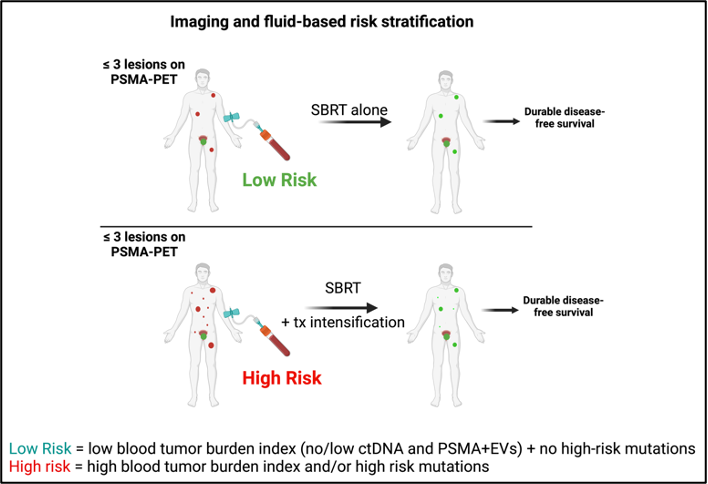
In conclusion, the ORIOLE and STOMP trials have established SBRT as the control arm in ongoing trials in omCSPC. In the experimental arm, therapy is being escalated with the addition of various systemic therapies to SBRT. These include but are not limited to Ra-223 (RAVENS), ADT (RADIOSA, NRG PROMETHEAN, PERSIAN, DIVINE/DEVIATE), 177Lu-PSMA (POPSTAR II, PSMA-DC), and immune checkpoint inhibitors (SBRT-AMICO). Andrews JR et al’ study supports the clinical utility of blood-based biomarkers to better estimate tumor burden and risk of disease progression in patients diagnosed with omCSPC. Besides PSMA+ EVs and gene mutations, circulating tumor DNA (ctDNA) has shown strong potential to risk-stratify patients with oligometastatic cancer pre-radiotherapy and to assess minimal residual disease post-treatment.6,7 Altogether, these recent findings support the integration of imaging- and fluid-based tools to stratify omCSPC patients into “low” vs. “high” risk in order to select which patients are likely to benefit from systemic therapy escalation from those who may benefit from SBRT alone (Figure 2).
Written by: Fabrice Lucien, PhD,1 Aadel A. Chaudhuri, MD, PhD,2,3 and Sean S. Park, MD, PhD3
- Department of Urology, Mayo Clinic, Rochester, MN, USA
- Department of Immunology, Mayo Clinic, Rochester, MN, USA
- Department of Radiation Oncology, Mayo Clinic, Rochester, MN, USA
- Ost, P., et al. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J Clin Oncol 36, 446-453 (2018).
- Phillips, R., et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol 6, 650-659 (2020).
- Deek, M.P., et al. Long-Term Outcomes and Genetic Predictors of Response to Metastasis-Directed Therapy Versus Observation in Oligometastatic Prostate Cancer: Analysis of STOMP and ORIOLE Trials. J Clin Oncol 40, 3377-3382 (2022).
- Andrews, J., et al. PSMA+ Extracellular Vesicles are a Biomarker for SABR in Oligorecurrent Prostate Cancer Analysis from the STOMP-like and ORIOLE trial cohorts. Clin Cancer Res (2025).
- Lucien, F., et al. Tumor-Derived Extracellular Vesicles Predict Clinical Outcomes in Oligometastatic Prostate Cancer and Suppress Antitumor Immunity. Int J Radiat Oncol Biol Phys (2022).
- Semenkovich, N.P., et al. Pre-radiotherapy ctDNA liquid biopsy for risk stratification of oligometastatic non-small cell lung cancer. NPJ Precis Oncol 7, 100 (2023).
- Pellini, B., et al. ctDNA MRD Detection and Personalized Oncogenomic Analysis in Oligometastatic Colorectal Cancer From Plasma and Urine. JCO Precis Oncol 5(2021).