We conducted a study in a large data set to further validate the ability of PSADT to predict clinical outcomes in nmCRPC and address the question: How does PSADT impact health care resource utilization (HCRU) and costs?6 We hypothesized that among men with nmCRPC, shorter PSADT would not only result in worse overall and metastasis-free survival (OS and MFS), but also greater economic impact.
We acquired patient data from between 2012 and 2016 from a large cohort of 2800 men from the Veterans Health Administration (VHA). We studied men with non-metastatic prostate cancer with at least two PSA increases after hormonal therapy. The third PSA measurement was the index date (i.e., the CRPC date) and patients had at least three post-index PSA measurements until disenrollment, study end, or death. We then grouped patients into the following 2-month cohorts based on post-index PSADT: ≤2 months; >2 to ≤4 months; >4 to ≤6 months; >6 to ≤8 months; >8 to ≤10 months; >10 months to ≤12 months; and the reference cohort, which was >12 months.
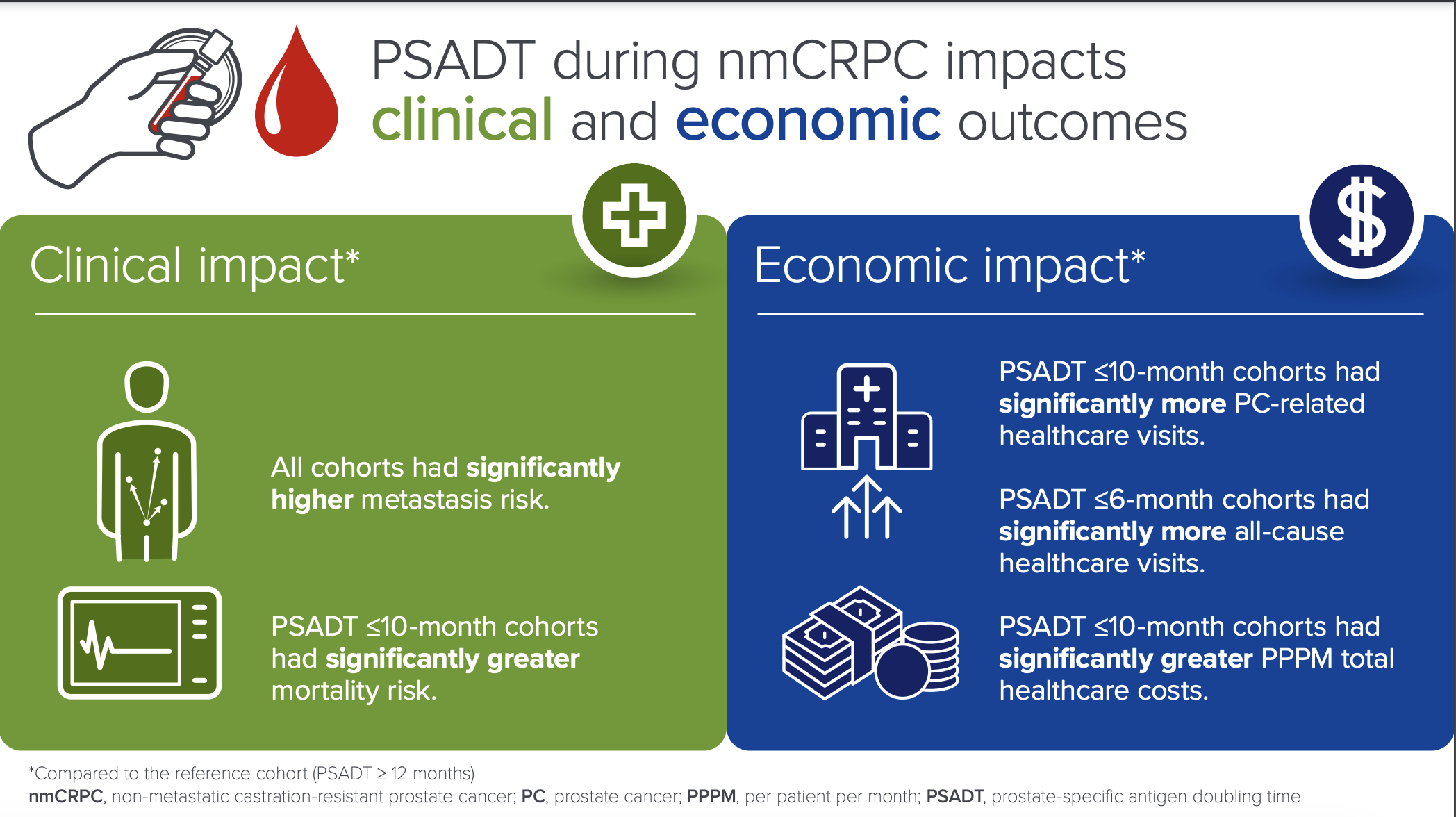
The median follow-up of the study was 30 months (~2.5 years) and the median PSADT was 17 months. 1670 patients (60%) comprised the reference group (>12 months). Relative to the reference group, all groups with shorter PSADT had higher metastasis risk. Similarly, all PSADT groups up to 10 months had shorter OS than the reference group and, although not statistically significant, the 10–12-month group also trended worse for OS than the reference group.
Notably, shorter PSADT was also associated with greater economic impact. We found that PSADT up to 10 months had greater prostate cancer related HCRU for health care visits relative to the reference group. HCRU included inpatient visits, inpatient length of stays, outpatient visits, and pharmacy visits. We further observed that PSADT up to 6 months had greater all-cause HCRU for health care visits relative to the reference group. Importantly, total health care costs per patient per month were also significantly greater for men with PSADT up to 10 months relative to the reference group.
This real-world retrospective study validates results from previous studies by showing that shorter PSADT is a strong predictor of worse clinical outcome in patients with nmCRPC.3–5 Importantly, our findings also show an inverse relationship between PSADT and economic outcomes. Due to its large patient sample size, this study was able to demonstrate for the first time that there are significant differences between 2-month intervals of PSADT in terms of risk of poor patient outcomes. The results of this study can help to better determine high-risk patients potentially eligible for novel hormonal therapy and conversely low-risk patients best served with conservative strategies to balance risks and costs.
Written by: Stephen J. Freedland, MD, Cedars-Sinai Medical Center, Los Angeles, CA
References:
- Sher HI, Halabi S, Tannock I, et al. Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the Prostate Cancer Clinical Trials Working Group. J Clin Oncol 2008;26:1148–1159.
- Gillessen S, Attard G, Beer TM, et al. Management of patients with advanced prostate cancer: report of the Advanced Prostate Cancer Consensus Conference 2019. Eur Urol 2020;77:508–547.
- Smith MR, Saad F, Oudard S, et al. Denosumab and bone metastasis-free survival in men with nonmetastatic castration-resistant prostate cancer: exploratory analyses by baseline prostate-specific antigen doubling time. J Clin Oncol 2013;31:3800–3806.
- Howard LE, Moreira DM, De Hoedt A, et al. Thresholds for PSA doubling time in men with non-metastatic castration-resistant prostate cancer. BJU Int 2017;120:e80–e86.
- Freedland SJ, Pilon D, Bhak RH, et al. Predictors of survival, healthcare resource utilization, and healthcare costs in veterans with non-metastatic castration-resistant prostate cancer. Urol Oncol 2020;38:930.e13–930.e21.
- Freedland SJ, Ramaswamy K, Huang A, et al. Survival and economic impact of rapid prostate-specific antigen doubling time in patients with nonmetastatic castration-resistant prostate cancer. Clin Genitourin Cancer 2023;S1558–7673(23)00022–8.
- Dr. Freedland reports consulting and honoraria to Astellas Pharma, AstraZeneca, Bayer, Exact Sciences, Janssen Biotech, Merck, Myovant Sciences, Pfizer, and Sanofi.
- Medical writing support was provided by Peter Gray of Onyx (a Prime Global agency) and funded by Pfizer Inc. and Astellas Inc.