Despite the substantial benefit seen with immune checkpoint inhibition using CTLA-4, PD-1, or PD-L1 antibodies in other types of cancers, as monotherapy, these agents have shown limited efficacy in prostate cancer. The use of candidate biomarkers to identify patients more likely to respond to immune checkpoint inhibition, such as PD-L1 expression, TMB, MSI, mismatch repair (MMR) deficiency, and defects in DNA damage repair such as CDK12 inactivating mutations, is under ongoing investigation. As another approach, several ongoing phase III trials in metastatic prostate cancer leverage the combination of immune checkpoint inhibition with other drugs such as enzalutamide, docetaxel, olaparib, and cabozantinib (Table 1).
Table 1. Ongoing phase III trials* of immune checkpoint inhibition in metastatic prostate cancer
* Accessed from https://ClinicalTrials.gov on July 10th, 2020.
Abbreviations: Abi – abiraterone acetate with prednisone; ADT – androgen deprivation therapy; Atezo – atezolizumab; Chemo – chemotherapy; Enza – enzalutamide; Ipi – ipilimumab; mCRPC – metastatic castration-resistant prostate cancer; mHSPC – metastatic hormone-sensitive prostate cancer; NHA – next-generation hormonal agent (abiraterone, enzalutamide, apalutamide, or darolutamide); Nivo – nivolumab; Pembro – pembrolizumab
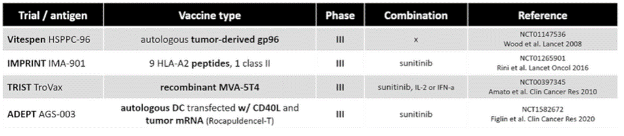
Another promising immuno-oncology approach involves leveraging phenotypic markers expressed by prostate cancer tumor cells to bypass the typical requirements for MHC class I interaction. Prostate-specific membrane antigen (PSMA) is one attractive target, and the degree of PSMA expression by prostate cancer tumor cells can be identified by next-generation PET imaging for individual patients. Bispecific antibodies, such as bispecific T cell engagers (BiTE®s), can be engineered to engage patients’ endogenous T cells while binding to tumor-specific antigens in an attempt to increase cytotoxic T cell infiltration into the tumor microenvironment. CAR-T cells use designer fusion proteins to identify and destroy cells bearing specific surface epitopes, with later-generation CARs using costimulatory molecules promoting the production of cytokines that assist with T cell activity. Experience with bispecific antibodies and CAR-T cell therapy in metastatic prostate cancer is limited, but phase I and II trials are ongoing (Table 2). We hope that the use of these novel and more targeted approaches can ultimately transcend the current limitations imposed by the immune-exclusive prostate cancer tumor microenvironment.
Table 2. Ongoing trials* of bispecific antibodies or CAR-T cell therapy in prostate cancer
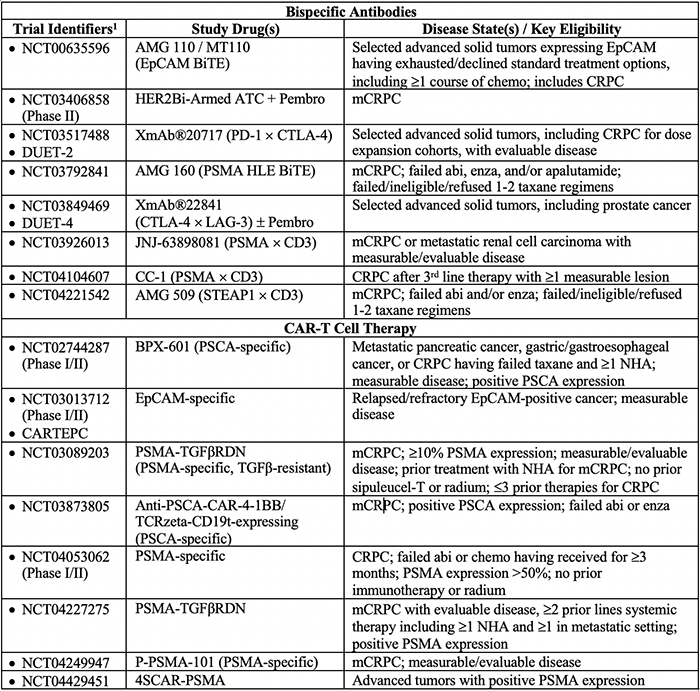
* Accessed from https://ClinicalTrials.gov on July 10th, 2020.
1All are phase I studies unless otherwise indicated.
Abbreviations: Abi – abiraterone; ATC – Activated T cells; BiTE – bi-specific T-cell engager; CAR-T – chimeric antigen receptor T-cells; chemo – chemotherapy; CRPC – castration-resistant prostate cancer; Enza – enzalutamide; HLE – half-life extended; mCRPC – metastatic castration-resistant prostate cancer; NHA – next-generation hormonal agent (abiraterone, enzalutamide, apalutamide, or darolutamide); Pembro - pembrolizumab
Written by: Risa L. Wong, MD and Evan Y. Yu, MD, University of Washington and Fred Hutchinson Cancer Research Center, Seattle, WA.
Read the Abstract