Penile squamous cell carcinoma (PSCC) is a rare malignancy in developed nations, with an annual incidence varying from 0.3 to 1 per 100,000 per year, accounting for approximately 0.4 to 0.6 % of all men malignancies (1).
Diagnosis is delayed in up to 50% of patients with PSCC because of shame, guilt, fear, ignorance and carelessness. This condition leads to two–thirds of the patients having an organ–confined disease at the time of initial diagnosis, whereas 30% of patiens present with locoregional or distant mestasis.
Primary metastatic sites are the regional inguinal lymph nodes (up to 45%, depending on the histological pattern) and later, the pelvic nodes. Detectable distant metastases (lung, liver, bone, or brain) are rare and occur late in the course of the disease (2,3).
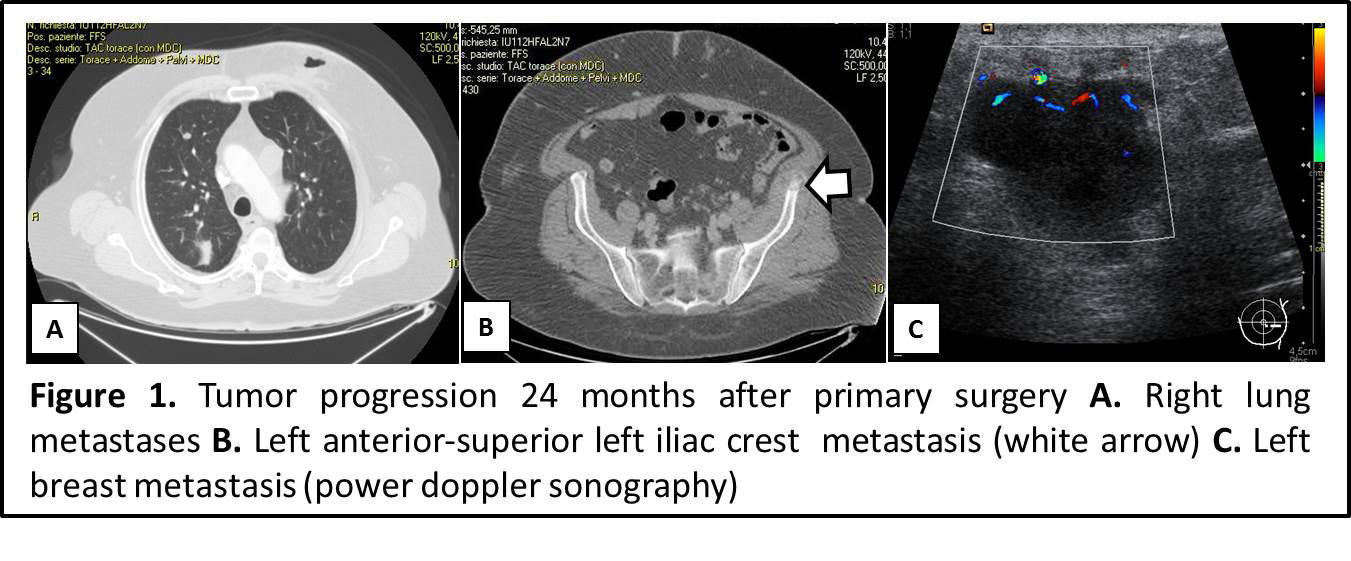
As showed in our report, two years after R0 surgical treatment and adjuvant chemotherapy for an inguinal node positive PSCC, the patient expierenced an aggressive tumoral progression with lung, bone and breast gland metastatization, an unusual tumoral progression (Figure 1).
Our patient underwent breast lumpectomy and adjuvant chemotherapy, achieving 6 months of clinical stability.
Thirty months after primary surgery, a full body CT scan showed massive progression of pulmonary dissemination, besides distant spreading to the anterior and posterior abdominal wall (Figure 2).

Tumoral progression caused patient’s death 2 months later.
This unique case shows PSSC as an unpredictable tumor with an extremely aggressive behavior in its distant spreading.
Low prevalence for similar cases, heterogeneous clinical appearance and different diagnostic-therapeutic strategies make it difficult to perform randomized trials. There is an overall low level of evidence leading to a complete abscence of uniform treatment guidelines.
Maximum effort must be done in PSSC patient’s clinical-instrumental follow up, in order to detect early tumoral relapsing (or progression) and to develop multicenter randomized trials.
Written By:
Alejandro Martin Sanchez M.D., Gianluca Franceschini M.D., Riccardo Masetti M.D.
Breast Unit, Catholic University of Sacred Heart – Rome, Italy.
REFERENCES
1. Bleeker MC, Heideman DA, Snijders PJ, Horenblas S, Dillner J, Meijer CJ. Penile cancer: epidemiology, pathogenesis and prevention. World J Urol. 2009 Apr;27(2):141-50.
2. Cubilla AL. The role of pathologic prognostic factors in squamous cell carcinoma of the penis. World J Urol. 2008; 27: 169–177.
3. He Y, Markelov A, Amani M. Penile cancer metastases to the groin. Arch Clin Exp Surg. 2014;3(1):56–8
Figure legends
Figure 1. Tumor progression 24 months after primary surgery A. Right lung metastases B. Left anterior-superior left iliac crest metastasis (white arrow) C. Left breast metastasis (power doppler sonography)
Figure 2. Tumor progression 36 months after primary surgery A. Multiple and bilateral lung metastases B. Right-anterior abdominal wall metastasis (white arrow) C. Left-posterior abdominal wall metastasis (white arrow)