As systemic therapies become more effective, a critical question has re-emerged: does surgery still have a role in patients with initially advanced or even unresectable disease? In our study, we sought to address this question by examining real-world outcomes of consolidative surgery following EVP therapy in a carefully selected cohort of patients with invasive bladder cancer and upper tract urothelial carcinoma.3 To our knowledge, this study represents one of the largest series to focus specifically on consolidative surgery following this now–standard-of-care regimen.
Several findings from our study are particularly noteworthy. First, our findings support the technical feasibility of surgery after EVP. Despite theoretical concerns regarding treatment-related fibrosis, immune-mediated tissue changes, or altered planes, we observed no major intraoperative complications and consistently achieved negative surgical margins. These results are reassuring and align with emerging experiences from immunotherapy-based neoadjuvant approaches in urothelial cancer and other genitourinary malignancies.
Second, we observed remarkably high rates of pathological response, including a 45% complete response rate and 59% overall downstaging. These findings underscore the depth of response achievable with EVP and are consistent with signals from recent clinical trials.1,2 Importantly, nodal clearance was achieved in the majority of clinically node-positive patients, highlighting the potential of systemic therapy to convert patients to surgically curable states. However, these encouraging oncologic outcomes must be interpreted in the context of patient selection. All patients in our cohort were carefully chosen through multidisciplinary evaluation, with favorable performance status and demonstrable response to systemic therapy. As such, our results should not be generalized to all patients receiving EVP but rather viewed as evidence supporting a strategy of selective surgical consolidation [Figure]. In addition, longer-term follow-up is required to validate the oncologic benefit of this approach.
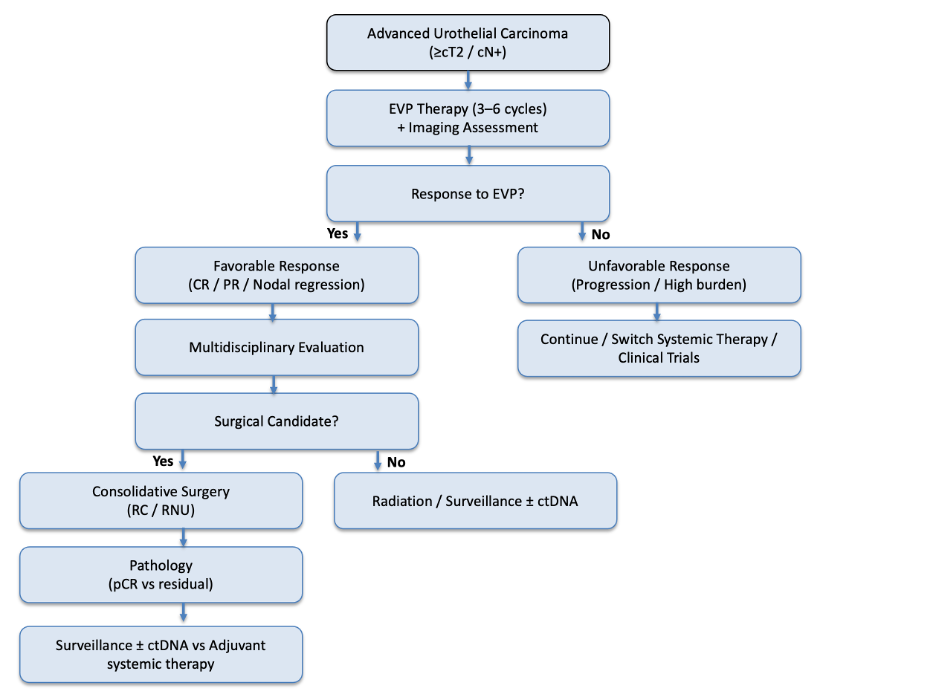
Figure: Clinical decision pathway for consolidative surgery after systemic therapy with enfortumab vedotin and pembrolizumab (EVP) for advanced urothelial carcinoma. CR: complete response; PR: partial response; RC: radical cystectomy; RNU: radical nephroureterectomy.
Third, while perioperative mortality was absent, postoperative morbidity remained substantial, with complication rates comparable to contemporary cystectomy and nephroureterectomy series. This emphasizes that, in the era of effective systemic therapy, radical surgery continues to carry significant risk and should be reserved for patients most likely to benefit. Thorough preoperative counseling is essential to balance the potential oncologic benefit of consolidative surgery against its associated morbidity.
An important emerging theme from our study is the role of circulating tumor DNA (ctDNA) as a complementary biomarker. In our limited cohort, ctDNA status correlated closely with clinical outcomes, suggesting a potential role in refining patient selection, guiding adjuvant therapy decisions, and improving surveillance strategies. As precision oncology advances, integration of molecular biomarkers may prove essential in optimizing multimodal treatment approaches.
Finally, our study highlights a broader conceptual shift: the re-integration of surgery into the management of advanced disease in the setting of highly active systemic therapy. Historically, surgery was pursued with curative intent for localized disease or for palliation in metastatic settings. However, with the advent of regimens such as EVP, the boundary between systemic and surgical management is becoming increasingly fluid. This paradigm, already established in malignancies such as renal cell carcinoma, may now be emerging in urothelial cancer.
Several critical questions remain unanswered. The optimal timing of surgery, the role of adjuvant therapy after response, the identification of patients most likely to derive durable benefit, the role of organ preservation in patients achieving complete response, and the integration of biomarkers such as ctDNA are all areas requiring prospective investigation. Ongoing phase III trials will be instrumental in defining these parameters and clarifying the survival impact of consolidative surgery in this setting.
In summary, our real-world experience suggests that consolidative surgery after EVP is not only feasible but may offer meaningful oncologic benefit in carefully selected patients. As systemic therapies continue to improve, multidisciplinary collaboration will be essential to identify those patients in whom surgery can transform a systemic response into a durable remission, or potentially, cure.
Written by: Alireza Ghoreifi,1 Ankeet Shah,2
- SUO Fellow, Department of Urology, Duke University, Durham, NC, USA
- Assistant Professor of Urology, Department of Urology, Duke University, Durham, NC, USA.
- Vulsteke C, Adra N, Danchaivijitr P, et al. Perioperative Enfortumab Vedotin and Pembrolizumab in Bladder Cancer. N Engl J Med 2026; 394: 1257–1269.
- Galsky MD, Valderrama BP, Maruzzo M, et al. Neoadjuvant and adjuvant enfortumab vedotin (EV) plus pembrolizumab (pembro) for participants with muscle-invasive bladder cancer (MIBC) who are eligible for cisplatin: Randomized, open-label, phase 3 KEYNOTE-B15 study. J Clin Oncol 2026; 44: LBA630–LBA630.
- Ghoreifi A, Hoimes CJ, Ramalingam S, et al. Outcomes of Consolidative Surgery Following Enfortumab Vedotin Plus Pembrolizumab for Advanced Urothelial Cancer: A Real-World Experience. Urol Oncol. 2026 Apr 3:111094.