The recent success of HER2-directed antibody-drug conjugates (ADCs), including trastuzumab deruxtecan and disitamab vedotin, has expanded the therapeutic landscape, yet beneath this momentum lies a fundamental problem: we still lack a clear and universally accepted definition of HER2 positivity in UC.
A matter of How: definitions and scoring inconsistencyThe magnitude of this challenge becomes evident when examining the heterogeneity of HER2 assessment across studies. Some studies adopt breast cancer criteria, requiring complete circumferential membrane staining;1-3 others use gastroesophageal junction (GEJ) criteria, where incomplete basolateral staining is sufficient;4 several studies employ modified institutional algorithms with limited external validation.5,6 These definitions come from tumors with profoundly different architectures and staining behaviors, and none of these frameworks were developed for urothelial carcinoma (Figure 1).7
Consequently, HER2 positivity rates reported in UC vary from as low as 4% to as high as 83%, depending largely on the scoring system applied rather than the underlying biology.8 A systematic review of 35 studies showed that HER2 positivity ranged from 6–37% when predefined criteria were used, and 4–83% when all scoring systems were included.9 The same tumor may be classified as HER2-positive under one system and HER2-negative under another. This issue has become increasingly relevant in the ADC era. DESTINY-PanTumor02 trial, which supported the tumor-agnostic approval of trastuzumab deruxtecan, adopted GEJ criteria and reported response rates approaching 60% among IHC3+ tumors.4 Yet many earlier UC trials defined HER2-positive as IHC3+ or IHC2+/FISH+, while others classified IHC1+ as “HER2-expressing,” particularly in ADC-focused studies. As a result, cross-trial comparisons become increasingly difficult, and the true prevalence of actionable HER2 remains uncertain .
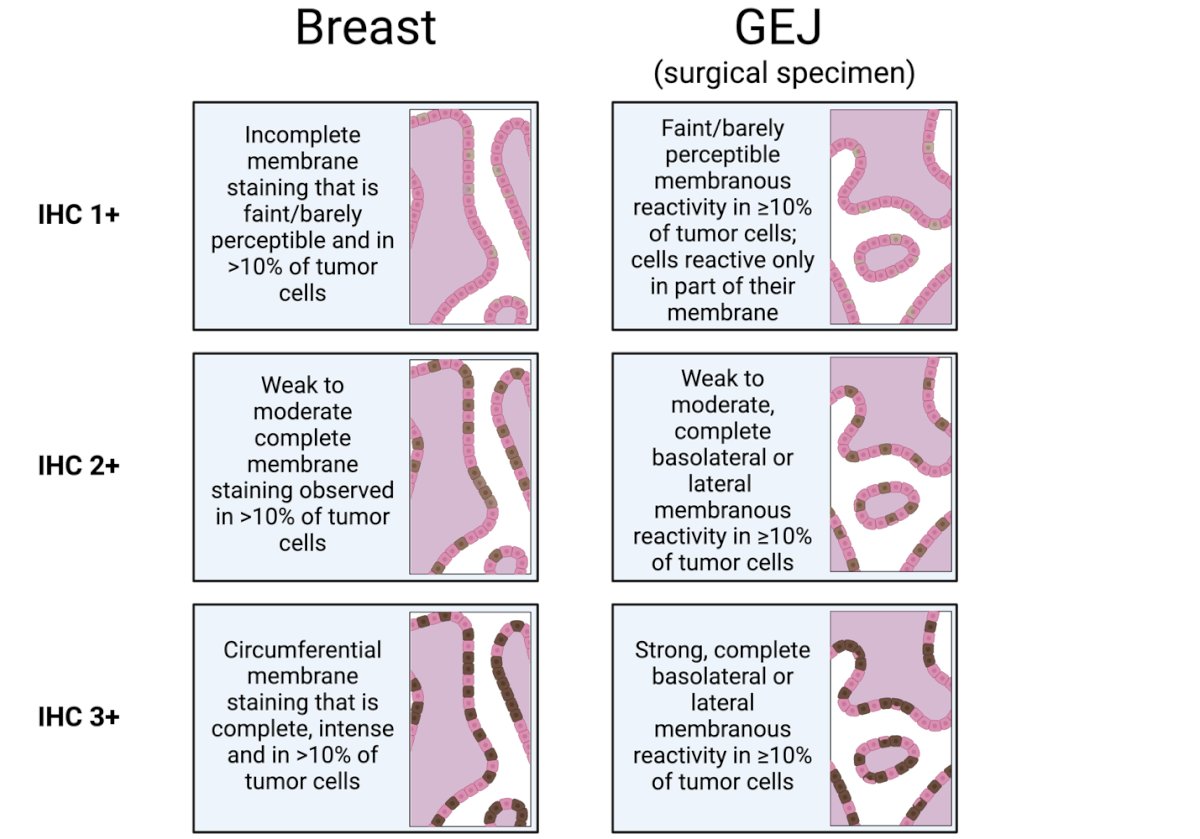
Figure 1: Comparative HER2 IHC Scoring Patterns in Breast and Gastro Esophageal Junction (GEJ)
Unsurprisingly, this variability yields results that are challenging to compare. These discrepancies underscore the need for a unified framework: a consensus definition of HER2 scoring and positivity specific to urothelial carcinoma.
A matter of When: the temporal and biological dynamics of HER2 expressionHER2 expression in UC is dynamic and discordance between primary tumors and metastatic lesions has been reported, with reports showing loss of HER2 in up to 55% of metastases relative to paired primary tumors. In upper tract UC, temporal shifts are even more pronounced, with HER2 status converting in roughly 73% of cases between primary and recurrent samples.10,11 Therapeutic pressure adds another layer of complexity. Evidence from metastatic breast cancer demonstrates that nearly one-third of patients lose HER2 expression after exposure to ADCs like trastuzumab deruxtecan.12 Similar selective pressures might be expected in UC for HER2. These shifts mean that archival samples may misclassify patients, particularly in later-line settings. Questions arise
- When is baseline truly baseline? at diagnosis, after platinum chemotherapy, immediately pre-ADC?
- Should HER2 be reassessed after exposure to modern frontline regimens?
- Can circulating tumor DNA complement tissue-based testing? Early results from HERALD demonstrate that clearance of ERBB2-amplified ctDNA correlates with response to T-DXd13
Perhaps the most important unanswered question is whether HER2 “positivity” itself remains the correct framework.
Traditional HER2-directed therapies relied on HER2 signaling dependence. ADCs operate differently. HER2 primarily functions as a docking receptor that enables intracellular delivery of a potent cytotoxic payload. Through bystander effects and payload diffusion, therapeutic activity can extend beyond HER2-overexpressing cells.
This biological distinction may explain why meaningful responses are observed in HER2-low tumors and raises the possibility that HER2 expression should be viewed as a continuum rather than a binary positive-versus-negative biomarker.
If this proves correct, the future challenge may not be determining whether a tumor is HER2-positive, but rather identifying the minimum level of HER2 expression required for meaningful therapeutic benefit.
The road aheadAs HER2-targeted ADCs enter earlier disease settings—e.g., perioperative DV combinations achieving pCR rates exceeding 63% in HER2-expressing MIBC3 —the timing of biomarker assessment becomes even more consequential. Without temporal standardization, patients might be both incorrectly included and incorrectly excluded from treatment.
Rapid expansion of HER2-directed trials amid definitional fragmentation may lead to a labyrinth of unanswered questions, rather than the guiding thread required for accurate classification, meaningful comparison, and ultimately clinical translation.
Written by:
- Emanuele Crupi, MD Department of GU Medical Oncology, University of Texas MD Anderson Cancer Center, Houston, TX, USA
- Daniele Raggi, MD Department of Medical Oncology, The Royal Marsden Hospital NHS Foundation Trust, London, UK
References:
- Hussain MHA, MacVicar GR, Petrylak DP, Dunn RL, Vaishampayan U, Lara PN, et al. Trastuzumab, paclitaxel, carboplatin, and gemcitabine in advanced human epidermal growth factor receptor-2/neu-positive urothelial carcinoma: results of a multicenter phase II National Cancer Institute trial. J Clin Oncol Off J Am Soc Clin Oncol. 1 giugno 2007;25(16):2218–24. doi:10.1200/JCO.2006.08.0994 PubMed PMID: 17538166.
- Wülfing C, Machiels JPH, Richel DJ, Grimm MO, Treiber U, De Groot MR, et al. A single-arm, multicenter, open-label phase 2 study of lapatinib as the second-line treatment of patients with locally advanced or metastatic transitional cell carcinoma. Cancer. 1 luglio 2009;115(13):2881–90. doi:10.1002/cncr.24337 PubMed PMID: 19399906.
- Sheng X, Wang L, He Z, Shi Y, Luo H, Han W, et al. Efficacy and Safety of Disitamab Vedotin in Patients With Human Epidermal Growth Factor Receptor 2-Positive Locally Advanced or Metastatic Urothelial Carcinoma: A Combined Analysis of Two Phase II Clinical Trials. J Clin Oncol Off J Am Soc Clin Oncol. 20 aprile 2024;42(12):1391–402. doi:10.1200/JCO.22.02912 PubMed PMID: 37988648; PubMed Central PMCID: PMC11095880.
- Meric-Bernstam F, Makker V, Oaknin A, Oh DY, Banerjee S, González-Martín A, et al. Efficacy and Safety of Trastuzumab Deruxtecan in Patients With HER2-Expressing Solid Tumors: Primary Results From the DESTINY-PanTumor02 Phase II Trial. J Clin Oncol. gennaio 2024;42(1):47–58. doi:10.1200/JCO.23.02005
- Hashimoto M, Fujita K, Tomiyama E, Fujimoto S, Adomi S, Banno E, et al. Immunohistochemical Analysis of HER2, EGFR, and Nectin-4 Expression in Upper Urinary Tract Urothelial Carcinoma. Anticancer Res. 1 gennaio 2023;43(1):167–74. doi:10.21873/anticanres.16146 PubMed PMID: 36585180.
- Banerji U, van Herpen CML, Saura C, Thistlethwaite F, Lord S, Moreno V, et al. Trastuzumab duocarmazine in locally advanced and metastatic solid tumours and HER2-expressing breast cancer: a phase 1 dose-escalation and dose-expansion study. Lancet Oncol. agosto 2019;20(8):1124–35. doi:10.1016/S1470-2045(19)30328-6 PubMed PMID: 31257177.
- Crupi E, Pederzoli F, Huddart RA, Cheng L, Raggi D. HER2 in urothelial cancer: clinical speed outpacing diagnostic clarity. Nat Rev Urol. 5 maggio 2026;1–3. doi:10.1038/s41585-026-01151-w
- Raggi D, Crupi E, Pederzoli F, Martini A, Briganti A, Alhalabi O, et al. HER2 and urothelial carcinoma: current understanding and future directions. Nat Rev Urol. 15 agosto 2025;1–23. doi:10.1038/s41585-025-01075-x
- Scherrer E, Kang A, Bloudek LM, Koshkin VS. HER2 expression in urothelial carcinoma, a systematic literature review. Front Oncol. 2022;12:1011885. doi:10.3389/fonc.2022.1011885 PubMed PMID: 36338710; PubMed Central PMCID: PMC9635895.
- Ye J, Liao X, Qiu Y, Wei Q, Bao Y. A systematic review and meta-analysis for human epidermal growth factor receptor 2 on upper tract urothelial carcinoma patients. Tumori J. 1 febbraio 2024;110(1):25–33. doi:10.1177/03008916231186178
- Grigg CM, Livasy C, He J, Hartman A, Clark PE, Zhu J, et al. Human epidermal growth factor receptor 2 overexpression is frequently discordant between primary and metastatic urothelial carcinoma and is associated with intratumoral human epidermal growth factor receptor 2 heterogeneity. Hum Pathol. gennaio 2021;107:96–103. doi:10.1016/j.humpath.2020.10.006 PubMed PMID: 33121981.
- Gouda MA, Gonugunta A, Dumbrava EE, Yap TA, Rodon J, Piha-Paul SA, et al. Human Epidermal Growth Factor Receptor 2 Loss following Treatment with Trastuzumab Deruxtecan in Patients with Metastatic Breast Cancer. Clin Cancer Res Off J Am Assoc Cancer Res. 1 aprile 2025;31(7):1268–74. doi:10.1158/1078-0432.CCR-24-3468 PubMed PMID: 39841861.
- Taniguchi H, Yagisawa M, Satoh T, Kadowaki S, Sunakawa Y, Nishina T, et al. Tissue-agnostic efficacy of trastuzumab deruxtecan (T-DXd) in advanced solid tumors with HER2 amplification identified by plasma cell-free DNA (cfDNA) testing: Results from a phase 2 basket trial (HERALD/EPOC1806). J Clin Oncol. giugno 2023;41(16_suppl):3014–3014. doi:10.1200/JCO.2023.41.16_suppl.3014