In this multicenter real-world study—the second largest series worldwide to date—we confirm that TMT achieves favorable oncological outcomes while preserving bladder function. Our findings reinforce that appropriate patient selection is critical, with factors such as tumor stage, completeness of resection, and baseline characteristics significantly impacting recurrence and survival.
Importantly, this study demonstrates the reproducibility of TMT across multiple institutions, supporting its implementation in routine clinical practice. These results position TMT not only as an alternative for unfit surgical candidates but as a valid curative strategy in well-selected patients.
Building on this work, our group is currently expanding the cohort to nearly 700 patients, with ongoing analyses comparing radiotherapy alone versus TMT, as well as outcomes in node-positive versus node-negative disease, among other key variables.
In conclusion, TMT represents a robust and scalable approach in MIBC, supported by high-level real-world evidence and continued research development.
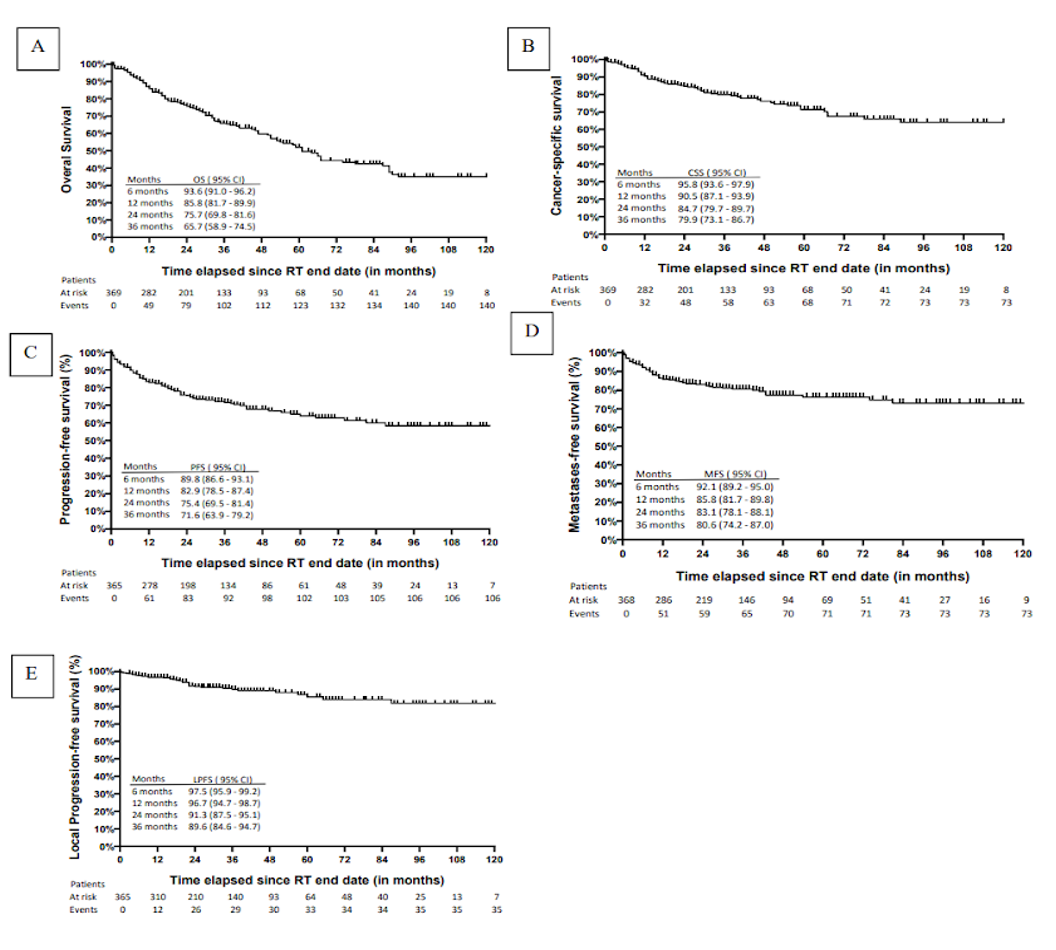
(A) Overall survival (OS), (B) cancer-specific survival (CSS), (C) progression-free survival (PFS), (D) metastasis-free survival (MFS), and (E) local progression-free survival (LPFS). Time zero was defined as the date of radiotherapy completion (last treatment fraction). Tick marks indicate censored observations. Numbers at risk and cumulative events are shown below each curve. Survival probabilities are reported at 6, 12, 24, and 36 months with 95% confidence intervals (CI). Curves were not extended beyond time points with fewer than 10 patients at risk.
Written by: Nicolás Feltes Benítez, MD, Radiation Oncologist, Hospital Universitario de Terrassa, Terrassa, Spain
Read the Abstract