However, only 30-40% of patients achieve pathological complete response to NAC, meaning the majority experience treatment-related toxicity and delays to surgery without benefit.2,3 Rarely, we have patients who progress in stage despite NAC at the time of final pathology. Identifying which patients will respond to NAC before initiating treatment would allow clinicians to personalize strategies and avoid unnecessary toxicity.
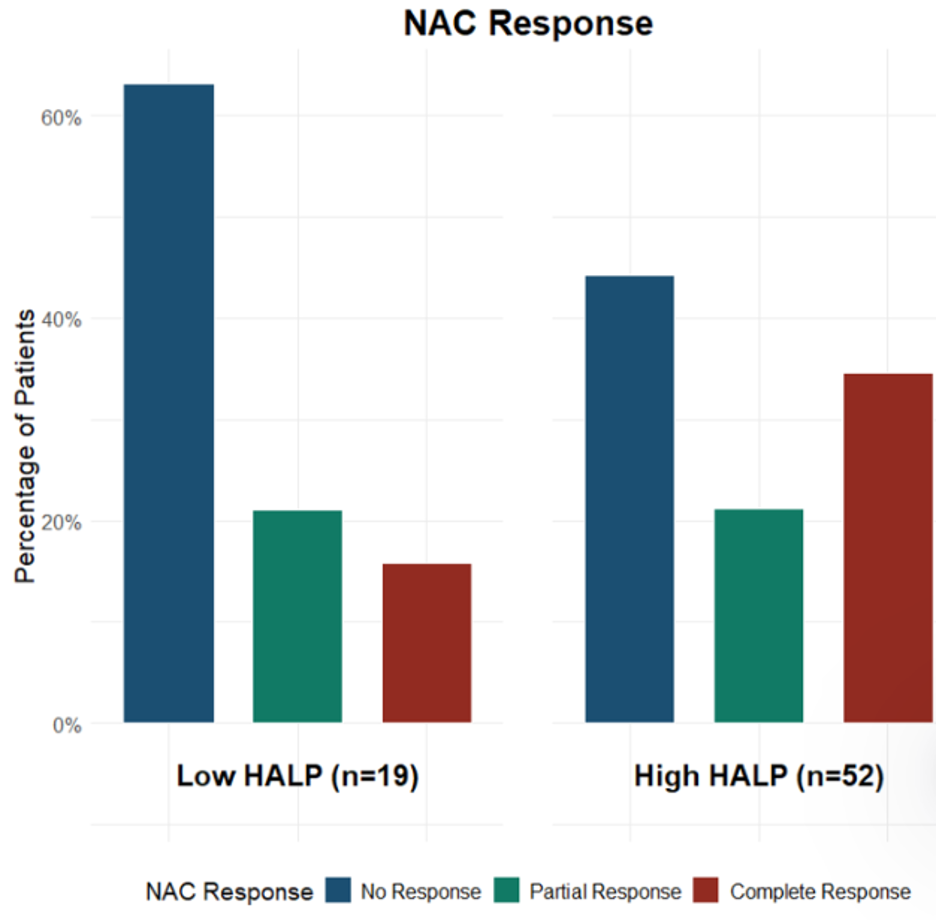
Our recent study investigated the hemoglobin, albumin, lymphocyte, and platelet (HALP) score as a predictor of NAC response in 70 MIBC patients.4 The HALP score is a composite inflammatory and nutritional biomarker calculated from routine pretreatment laboratory values: (hemoglobin × albumin × lymphocyte count) / platelet count. We identified an optimal cutoff value of 25.0, stratifying patients into Low HALP (N=18) and High HALP (N=52) groups. The findings were interesting: patients in the Low HALP group demonstrated a 66.7% rate of non-response to NAC compared to 44.2% in the High HALP group, while the High HALP group achieved a complete response rate of 34.6%, more than double the 16.7% rate in the Low HALP group. Patients in the High HALP group had a 2.1 times greater likelihood of achieving a complete response.4
The clinical importance of identifying NAC responders and non-responders extends beyond academic interest. For the 60-70% of patients who do not achieve a complete response, NAC represents treatment-related toxicity, disease progression, and delay to surgery without benefit.2,3 Cisplatin-based chemotherapy carries significant risks, including nephrotoxicity, ototoxicity, peripheral neuropathy, and myelosuppression.5 The HALP score’s ability to identify patients with a 66.7% likelihood of non-response could enable clinicians to counsel these patients about alternative strategies, including proceeding directly to radical cystectomy or alternative agents. Having said that, the authors understand that this is a mere initial step in shifting the needle towards better stratification and that this article is not practice-changing.
The timing of radical cystectomy after NAC represents another critical consideration. Current guidelines recommend performing cystectomy within 8-12 weeks of completing NAC.6 However, recent evidence suggests that delays beyond this window are associated with worse oncological outcomes.7,8 For patients identified as likely non-responders by low HALP scores, these findings support proceeding directly to radical cystectomy without NAC, avoiding both treatment-related toxicity and oncological risks associated with delayed surgery.
The landscape of perioperative therapy for MIBC is undergoing a fundamental transformation with the recent FDA approval of enfortumab vedotin-pembrolizumab (EV-P) in November 2025.9 This approval was based on the EV-302/KEYNOTE-A39 trial, which demonstrated that EV-P significantly improved overall survival compared to platinum-based chemotherapy, with a median overall survival of 31.5 months versus 16.1 months.10 The combination of enfortumab vedotin, an antibody-drug conjugate targeting Nectin-4, with pembrolizumab, a PD-1 checkpoint inhibitor, represents a mechanistically distinct approach and offers new hope for patients who are cisplatin-ineligible or might not respond to conventional NAC.
The integration of predictive biomarkers like the HALP score becomes critical in this evolving treatment landscape. As clinicians now have multiple perioperative treatment options—cisplatin-based NAC, EV-P, or direct cystectomy—the ability to stratify patients according to their likelihood of response will be essential. The HALP score’s foundation in inflammatory and nutritional status may reflect fundamental aspects of tumor biology and host immune function that influence response to both chemotherapy and immunotherapy.11,12 Patients with low HALP scores may have compromised immune function that impairs response to conventional chemotherapy. Whether these patients might respond differently to immunotherapy-based combinations like EV-P remains an important question.
Several limitations warrant discussion. The retrospective design and small sample size (N=70) limit generalizability. The optimal HALP cutoff of 25.0 was derived from this cohort; external validation is essential. The study period predates EV-P availability. We did not evaluate other emerging biomarkers such as circulating tumor DNA, molecular subtypes, or radiomics features, which may provide complementary predictive information.13,14,15
Future research should focus on several key directions. Comparative studies will help determine whether integrated multi-biomarker models offer superior performance.13,14,15 Investigation of whether the HALP score or other biomarkers predict response to EV-P will be critical. Clinical trials incorporating validated biomarkers into treatment allocation algorithms will be necessary to demonstrate improved outcomes.
The HALP score represents a promising, readily available tool for predicting NAC response in MIBC patients. Its calculation from routine pretreatment laboratory values makes it immediately accessible. The finding that low HALP scores identify patients with a 66.7% likelihood of non-response has important implications for treatment selection. Recent studies have identified several other promising predictive biomarkers. Deol et al. (2024) demonstrated that B7-H3 expression may predict NAC response in MIBC.16 Hensley et al. (2019) showed that phenotypic signatures could predict response to cisplatin-based NAC.17 Hepburn et al. (2021) identified CNGB1 as a predictor of NAC response.18 Additionally, immune-related biomarkers, including B cell function genes (CD19, CLEC4D, CXCR5), dendritic cell activation markers (XCR1, CCL5), and tertiary lymphoid structures, have been associated with pathological complete response.19 However, most of these biomarkers require specialized testing, limiting their widespread clinical implementation. As we move toward personalized approaches to MIBC management, integrating readily accessible predictive biomarkers like the HALP score with emerging therapies like EV-P offers the potential to optimize outcomes. This work highlights the need for continued investigation of predictive biomarkers to guide personalized treatment strategies in muscle-invasive bladder cancer.
Written by: Nassib Heidar, MD, University of Virginia School of Medicine, Charlottesville, VA
References:
- Russell, B., Liedberg, F., Khan, M. S., Nair, R., Thurairaja, R., Malde, S., Kumar, P., & Bryan, R. T. (2020). A systematic review and meta-analysis of delay in radical cystectomy and the effect on survival in bladder cancer patients. European Urology Oncology, 3(2), 239-249. https://doi.org/10.1016/J.EUO.2019.09.008
- Murphy, W. M., Takezawa, K., & Maruniak, N. A. (2022). Interobserver discrepancy using the 1998 World Health Organization/International Society of Urologic Pathology classification of urothelial neoplasms: practical choices for patient care. The Journal of Urology, 168(3), 968-972. https://doi.org/10.1016/S0022-5347(05)64548-6
- Tripathi, A., Plimack, E. R., & Geynisman, D. M. (2023). Predictors of response to neoadjuvant therapy in urothelial cancer. Critical Reviews in Oncology/Hematology, 192, 104236. https://doi.org/10.1016/j.critrevonc.2023.104236
- Stempel, J. M., Klaassen, Z., Wallis, C. J. D., Mossanen, M., Sood, A., Kibel, A. S., Trinh, Q. D., & Menon, M. (2026). Implications of hemoglobin, albumin, lymphocyte, platelet (HALP) score as a predictor of neoadjuvant chemotherapy response in bladder cancer patients. Urologic Oncology: Seminars and Original Investigations, 44(3), 111005. https://doi.org/10.1016/j.urolonc.2026.111005
- Galsky, M. D., Hahn, N. M., Rosenberg, J., Sonpavde, G., Hutson, T., Oh, W. K., Dreicer, R., Vogelzang, N., Sternberg, C. N., Bajorin, D. F., & Bellmunt, J. (2012). Treatment of patients with metastatic urothelial cancer “unfit” for Cisplatin-based chemotherapy. Journal of Clinical Oncology, 30(17), 2037-2044. https://doi.org/10.1200/JCO.2011.38.8123
- Chang, S. S., Bochner, B. H., Chou, R., Dreicer, R., Kamat, A. M., Lerner, S. P., Lotan, Y., Meeks, J. J., Michalski, J. M., Morgan, T. M., Quale, D. Z., Rosenberg, J. E., Zietman, A. L., & Holzbeierlein, J. M. (2017). Treatment of non-metastatic muscle-invasive bladder cancer: AUA/ASCO/ASTRO/SUO guideline. The Journal of Urology, 198(3), 552-559. https://doi.org/10.1016/j.juro.2017.04.086
- Nuijens, A. C., van Rooijen, K. L., Zuiverloon, T. C. M., Hendricksen, K., Boormans, J. L., & Aben, K. K. H. (2024). Longer time to radical cystectomy in patients treated with neoadjuvant chemotherapy is associated with worse oncological outcomes. Urologic Oncology: Seminars and Original Investigations, 42(3), 73.e1-73.e8. https://doi.org/10.1016/j.urolonc.2023.12.014
- Park, J., Kim, S., Jeong, I. G., Song, C., Hong, J. H., Kim, C. S., & Ahn, H. (2016). A retrospective analysis of the effect on survival of time from diagnosis to neoadjuvant chemotherapy to cystectomy for muscle invasive bladder cancer. The Journal of Urology, 195(4), 880-885. https://doi.org/10.1016/J.JURO.2015.11.024
- U.S. Food and Drug Administration. (2025, November 21). FDA approves pembrolizumab with enfortumab vedotin-ejfv for muscle invasive bladder cancer. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-pembrolizumab-enfortumab-vedotin-ejfv-muscle-invasive-bladder-cancer
- Powles, T., Valderrama, B. P., Gupta, S., Bedke, J., Kikuchi, E., Hoffman-Censits, J., Iyer, G., Vulsteke, C., Park, S. H., Shin, S. J., Castellano, D., Fornarini, G., Li, J. R., Gümüş, M., Mar, N., Loriot, Y., Fléchon, A., Duran, I., Drakaki, A., … Rosenberg, J. E. (2025). EV-302: Updated analysis from the phase 3 global study of enfortumab vedotin in combination with pembrolizumab (EV+P) vs chemotherapy (chemo) in previously untreated locally advanced or metastatic urothelial carcinoma (la/mUC) [Abstract 664]. Journal of Clinical Oncology, 43(5_suppl), 664. https://doi.org/10.1200/JCO.2025.43.5_suppl.664
- Guo, Y., Cai, K., Mao, S., Zhang, J., Wang, L., Zhang, Z., Liu, W., & Wang, G. (2021). Preoperative C-reactive protein/albumin ratio is a significant predictor of survival in bladder cancer patients after radical cystectomy: a retrospective study. Cancer Management and Research, 13, 8785-8797. https://doi.org/10.2147/CMAR.S338849
- Kang, M., Jeong, C. W., Kwak, C., Kim, H. H., & Ku, J. H. (2019). Preoperative neutrophil-lymphocyte ratio can significantly predict mortality outcomes in patients with non-muscle invasive bladder cancer undergoing transurethral resection of bladder tumor. Oncotarget, 10(12), 1345-1359. https://doi.org/10.18632/oncotarget.28302
- Pérez, M. J., Sánchez-Alcoholado, L., Jiménez-Cortegana, C., Alba, G., Cabeza-Segura, M., Ortega-Sánchez, M., Cantero-Cid, R., Fernández-Rueda, J. L., Villalba-Esparza, M., Becerra-Massare, P., Rodríguez-Serrano, E. M., Álvarez-Kindelán, J., Sánchez-Margalet, V., & de la Cruz-Merino, L. (2025). Biomarker-based nomogram to predict neoadjuvant chemotherapy response in muscle-invasive bladder cancer. Biomedicines, 13(3), 740. https://doi.org/10.3390/biomedicines13030740
- Sjödahl, G., Abrahamsson, J., Holmsten, K., Bernardo, C., Chebil, G., Eriksson, P., Johansson, I., Lindh, C., Lövgren, K., Liedberg, F., Patschan, O., Månsson, W., & Höglund, M. (2021). Different responses to neoadjuvant chemotherapy in urothelial carcinoma molecular subtypes. medRxiv. https://doi.org/10.1101/2021.05.11.21255912
- Cha, K. H., Hadjiiski, L. M., Samala, R. K., Chan, H. P., Cohan, R. H., Caoili, E. M., Paramagul, C., Alva, A., & Weizer, A. Z. (2017). Bladder cancer treatment response assessment in CT using radiomics with deep-learning. Scientific Reports, 7(1), 8738. https://doi.org/10.1038/s41598-017-09315-w
- Deol, A. D., Heath, E. I., Fontana, J. A., Lew, M., Smith, D., Grignon, D. J., & Tekyi-Mensah, S. (2024). B7-H3 expression predicts response to neoadjuvant chemotherapy in muscle-invasive bladder cancer. Urologic Oncology: Seminars and Original Investigations, 42(8), 252.e1-252.e8. https://doi.org/10.1016/j.urolonc.2024.04.012
- Hensley, P. J., Panebianco, V., Pietzak, E., Kutikov, A., Vikram, R., Galsky, M. D., Shariat, S. F., Rouprêt, M., Kamat, A. M., Xylinas, E., Psutka, S. P., Seiler, R., Black, P. C., & Lotan, Y. (2019). Contemporary staging for muscle-invasive bladder cancer: accuracy and limitations. European Urology Oncology, 2(3), 293-298. https://doi.org/10.1016/j.euo.2019.01.003
- Hepburn, A. C., Steele, R. E., Veeratterapillay, R., Wilson, L., Kounatidou, E., Barnard, A., Berry, P., Cassidy, J. R., Moad, M., El-Sherif, A., Gaughan, L., Robson, C. N., Heer, R., & Dykhuizen, E. C. (2021). The induction of core pluripotency master regulators in cancers defines poor clinical outcomes and treatment resistance. Oncogene, 40(4), 753-768. https://doi.org/10.1038/s41388-020-01574-3
- Ascierto, M. L., Idowu, M. O., Zhao, Y., Khalak, H., Payne, K. K., Wang, X. Y., Dumur, C. I., Bedognetti, D., Tomei, S., Ascierto, P. A., De Giorgi, V., Wang, E., Marincola, F. M., & Manjili, M. H. (2023). Molecular signatures mostly associated with NK cells are predictive of relapse-free survival in breast cancer patients. Journal of Translational Medicine, 11, 145. https://doi.org/10.1186/1479-5876-11-145