In the current study, we evaluated the long-term survival outcomes in this patient population, particularly of those NMIBC patients who were upstaged on the final radical cystectomy pathology.
Overall, 355 patients from three high-volume centers from 2004 to 2022 were included; among them, 58.87% (209 patients) received an ileal conduit, 40.28% (143 patients) had a neobladder, and 0.6% (2 patients) underwent cutaneous ureterostomy. The median follow-up was 37 months (IQR 10-75).
Disease upstaging to MIBC or node-positive disease was noted in 95 patients (34.4%). Perioperative outcomes, including the type of urinary diversion, operative time, estimated blood loss, transfusions, length of stay, reoperations, and early or late readmissions, did not differ significantly between the groups. The upstaged group had a higher incidence of Clavien Grade III late complications (p=0.004). Positive soft tissue margins (p<0.001) and recurrence rate, both local and distant (p=0.0), were significantly higher in upstaged patients.
On multivariable analysis, older age (≥83 years, odds ratio [OR]=19.7), presence of carcinoma-in-situ (CIS) combined with Ta/T1 disease (OR=2.7), and variant histology (OR=6.2) were found as predictors of pathological upstaging. Conversely, higher BMI (≥28 kg/m², OR=0.4) and isolated Tis disease (OR=0.1) were protective factors.
Survival analysis extending up to 12 years demonstrated that overall survival (OS) was significantly lower in the upstaged group (39%) than in those not upstaged (52%) (Figure 1), and cancer-specific survival (CSS) was higher among non-upstaged patients (79%) than among upstaged patients (68%) (Figure 2).
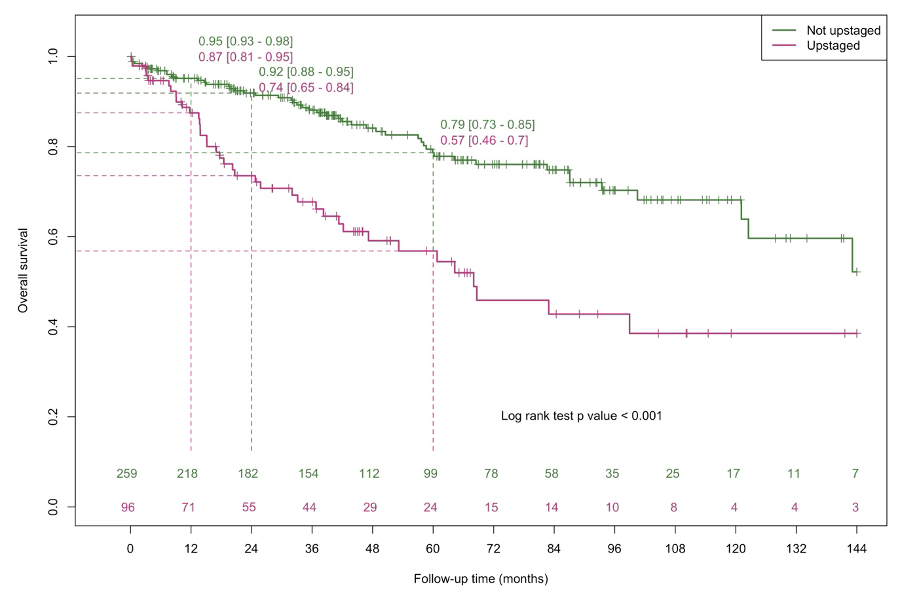
Figure 1: Comparison of overall survival of patients with NMIBC stratified according to disease upstaging vs no upstaging on final pathology.
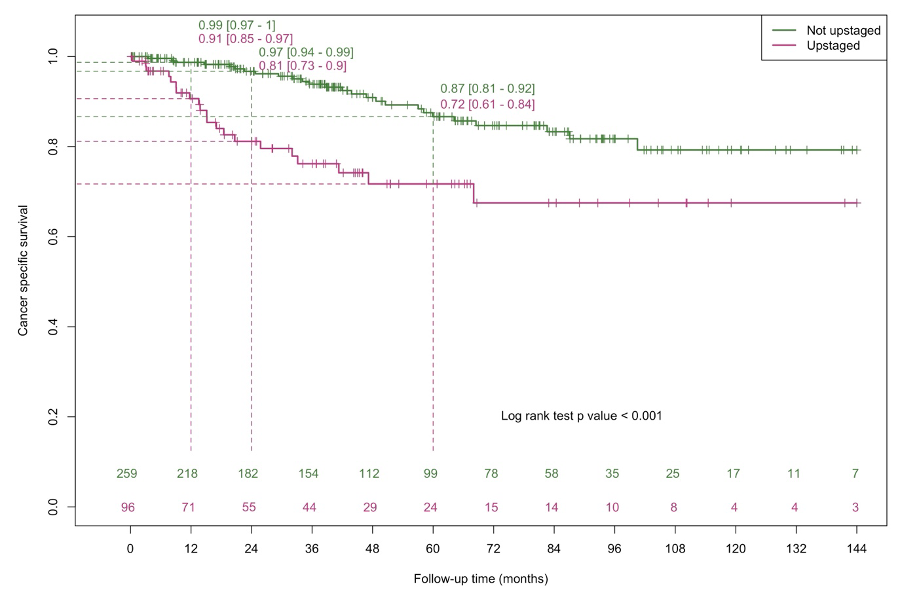
Figure 2: Comparison of cancer-specific survival of patients with NMIBC stratified according to disease upstaging vs no upstaging on final pathology.
Interestingly, there were no statistically significant differences in OS (p=0.29) and CSS (p=0.67) between patients who received BCG therapy before cystectomy and those who did not. This may be due to a large cohort of patients with high-risk features undergoing early cystectomy. The choice of urinary diversion evolved over the study period due to changes in surgical techniques, patient preferences, and increased experience with complex reconstructions like the neobladder (shown in supplementary figures).
NMIBC patients with high-risk characteristics may present with or progress to BCG-unresponsiveness, necessitating escalated therapeutic approaches. Contemporary guidelines recommend intravesical nadofaragene firadenovac, nogapendekin-α inbakicept, or systemic pembrolizumab for managing these cases. However, only approximately one-third of patients with BCG-refractory disease achieve a complete response in one year, underscoring the need for early radical cystectomy in most cases. While considering bladder-sparing approaches for high-risk bladder cancer, it is crucial to account for the risk of upstaging and nodal metastasis by opting for the least morbid yet oncologically safe surgical approach.
In conclusion, our study highlights the need for improved diagnostic techniques with imaging studies such as MRI and potential molecular markers such as circulating tumor DNA (ctDNA). Factors like CIS and variant histology should prompt clinicians to consider aggressive management strategies in the context of bladder-sparing approaches, given the significant risk of upstaging and poorer survival outcomes. RARC with ICUD offers a minimally invasive surgical option that has demonstrated robust long-term oncologic outcomes in appropriately selected NMIBC patients.
Written by: Neeraja Tillu, MD, Reuben Ben-David, MD, and Peter Wiklund, MD, PhD
- Department of Urology, Icahn School of Medicine at Mount Sinai Hospital, NY