To address this question, we assembled an international, multi-center retrospective cohort of BCG-unresponsive bladder cancer patients. Current thought remains that in concurrent T1 and CIS disease, the T1 component drives oncologic behavior while in concurrent Ta and CIS disease, the CIS component drives oncologic behavior. As a result, our team sorted patients by tumor stage as follows: T1 +/- CIS, Ta alone, and CIS +/- Ta. Oncologic outcomes were compared between these groups, and exploratory analyses further compared T1 alone versus Ta alone versus CIS ± T1/Ta and T1/Ta alone versus CIS ± T1/Ta.
Of 401 BCG-unresponsive NMIBC patients who underwent BST at 10 academic centers, 137 (34%) were T1 +/- CIS, 104 (26%) Ta alone, and 160 (40%) CIS +/- Ta. Disease progression (p<0.001), metastasis (p<0.001), and bladder cancer mortality (p=0.009) occurred more often in the T1 +/- CIS group versus Ta alone and CIS +/- Ta groups. Cystectomy occurred most often in the CIS +/- Ta and T1 groups (p=0.002). Exploratory analysis comparing T1 alone versus Ta alone versus CIS ± T1/Ta yielded similar findings. However, many of these differences were mitigated when comparing papillary disease only to any CIS as there were no significant differences in metastasis, bladder cancer mortality, or all-cause mortality.
The findings from this study highlight the worsened outcomes associated with T1 disease compared to Ta and CIS, both of which display less aggressive features. A trial of BST in the carefully selected Ta alone or CIS +/- Ta patient may not compromise oncologic outcomes. Importantly, the masking of oncologic differences when consolidating all papillary disease during comparison with any CIS suggests that linking all papillary patients into a singular group, as commonly done in clinical trial settings, is inappropriate. Ta disease appears more likely to evolve similarly to CIS disease rather than T1 disease and should be managed accordingly. Lastly, radical cystectomy appears to be most driven by the presence of CIS. While they should be interpreted in the context of likely selection bias in a retrospective cohort, these findings provide valuable insights into the role of tumor stage in BCG-unresponsive NMIBC and subsequent management.
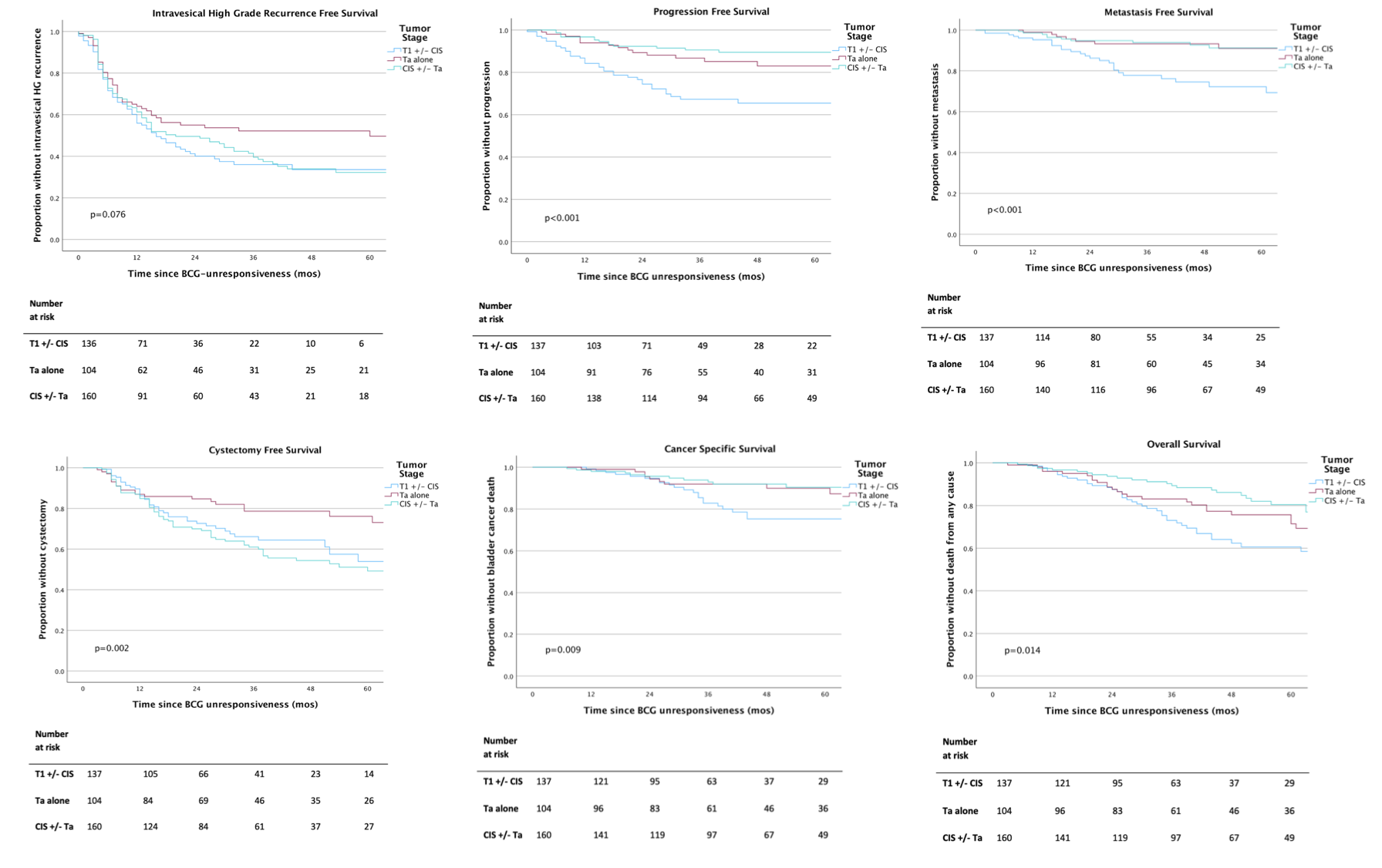
Figure A-F: Oncologic outcomes of BCG-unresponsive NMIBC patients undergoing at least 1 BST, stratified by tumor stage at initial BCG unresponsiveness, comparing T1 +/- CIS, Ta alone, and CIS +/- Ta. Kaplan-Meier curves showing intravesical high-grade recurrence free survival (A) progression free survival (B) metastasis free survival (C) cystectomy free survival (D) cancer specific survival (E) and overall survival (F), of BCG-unresponsive NMIBC patients. Abbreviations: BCG, bacillus Calmette-Guérin; NMIBC, non-muscle invasive bladder cancer.
Written by: Drupad Annapureddy, Jacob I. Taylor, MD, and Yair Lotan, MD, UT Southwestern Medical Center, University of Texas, Dallas, TX
Read the Abstract