This study explored the outcomes of patients with IR-NMIBC who received intravesical BCG or Gem/Doce for treatment. Notably, our study population was composed primarily of patients with TaHG disease. Patients with no evidence of recurrence after induction therapy were offered maintenance regimens. Patients received routine surveillance cystoscopies to assess for recurrence after treatment. Of 483 patients receiving intravesical treatment for NMIBC between 2013 – 2023, the analysis identified and included 127 IR-NMIBC patients (66 BCG and 61 Gem/Doce). In patients with primary TaHG disease, BCG had higher 2-yr high-grade RFS (80.9% [95% CI 69.1-94.8%]) compared to Gem/Doce (61.1% [95% CI 43.7-85.4%]) (log-rank, p = 0.027). The 2-yr any-grade RFS was superior for BCG (59.8% [95% CI 48.6-73.4%]) compared to Gem/Doce (40.9% [95% CI 28.4-59%]) (log-rank, p = 0.0036). Treatment with Gem/Doce was associated with a higher risk of high-grade recurrence in primary high-grade tumors (HR 3.4 [95% CI 1.27-9.1], p = 0.015) and a higher risk of any-grade recurrence (HR 1.87 [95% CI 1.1-3.2], p = 0.035). Receipt of maintenance therapy was associated with lower any-grade recurrence (HR 0.4, [95% CI 0.22-0.72], p = 0.002).
Previous studies have demonstrated comparable RFS between Gem/Doce and BCG in the IR-NMIBC group; however, significant differences exist between these studies and ours. First, our study mainly comprised solitary TaHG disease, while the other studies had primary or recurrent TaLG disease. Second, our maintenance therapy for Gem/Doce was similar to the 1-year maintenance therapy given with BCG; in prior studies, maintenance therapy was given for 2 years. This may explain why any-grade RFS curves are similar between the treatment arms up to one year, after which they begin to separate, thus highlighting the importance of maintenance regimens for patients receiving Gem/Doce. This difference can be further explained by the mechanism of action of these two therapies; while BCG provides a sustained immune response, Gem/Doce acts by direct cytotoxicity, which is subject to attrition without regular maintenance doses.
In summary, our study demonstrates that BCG is superior to Gem/Doce in patients with IR-NMIBC. With the widespread adoption of Gem/Doce, standardization of treatment protocols and mandated use of maintenance therapies is necessary to achieve outcomes comparable to the gold standard intravesical treatment, BCG. Future randomized controlled trials such as the BRIDGE (NCT05538663) will help shed more light on the comparative effectiveness of these two intravesical therapies and will guide the standardization of guidelines and treatment protocols.

Figure 1: Mechanism of action of Bacillus Calmette-Guérin (BCG) and sequential Gemcitabine/Docetaxel (Gem/Doce) for the treatment of localized non-muscle-invasive bladder cancer
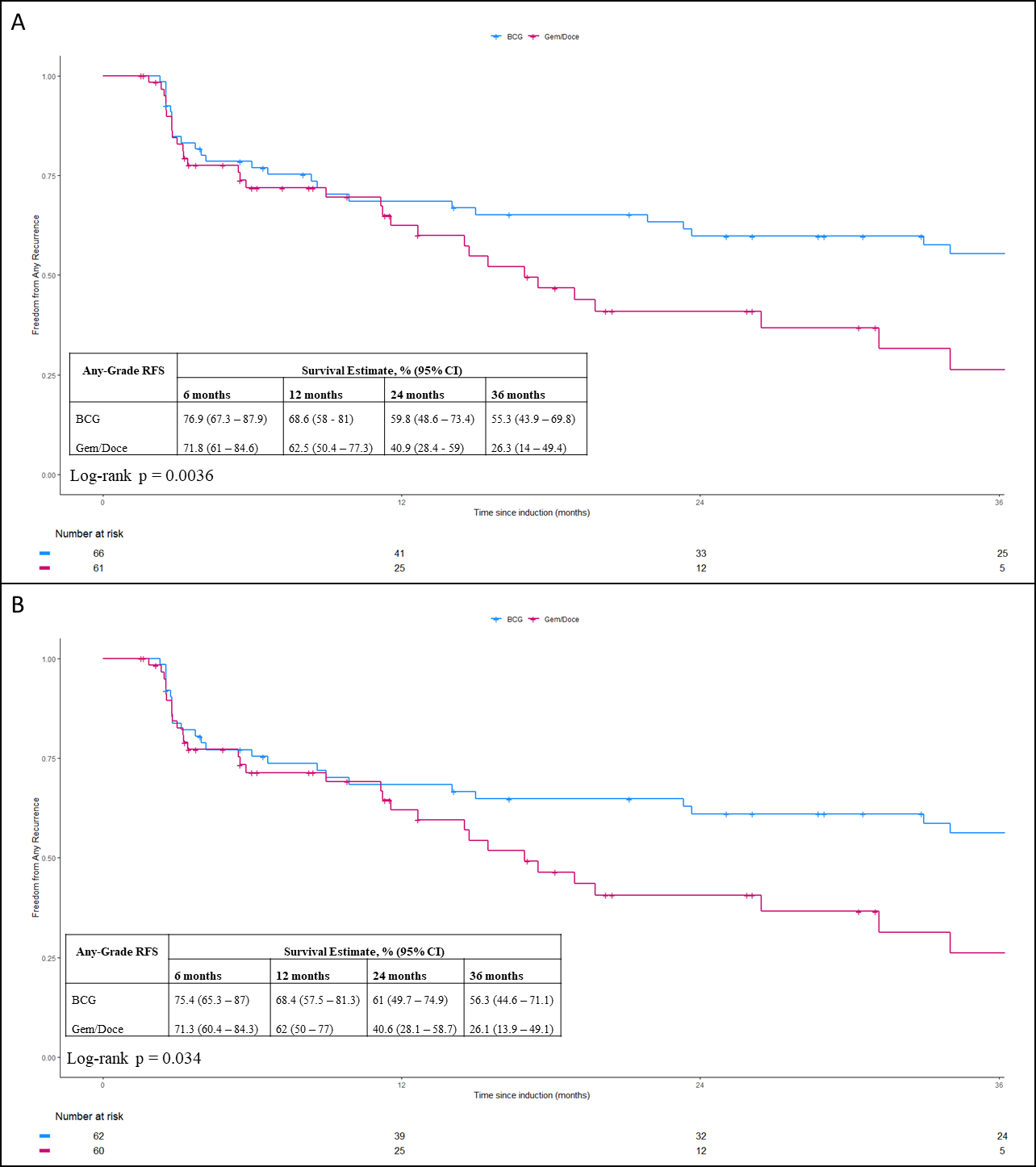
Figure 2: Any-Grade Recurrence-Free Survival (RFS) of patients receiving Bacillus Calmette-Guérin (BCG) and Sequential Intravesical Gemcitabine and Docetaxel (Gem/Doce) for AUA (A) and EAU (B) intermediate-risk non-muscle-invasive bladder cancer
Written by: Kaushik P. Kolanukuduru, Reuben Ben-David, & John P. Sfakianos
Department of Urology, Icahn School of Medicine at Mount Sinai. New York, NY
Read the Abstract