2. Maintenance of hygiene, particularly of the hands and perineum.
- Hands should be thoroughly washed before attempting catheterization
- The genitalia should be washed daily with soap and water and always cleansed from front to back
- Preferable to perform catheterization before bowel program to minimize bowel bacteria contamination of the urethra
- Immediate perineal hygiene in women is recommended after vaginal intercourse as the act of intercourse may push anal bacterial into the urethra. Avoidance of spermicidal lubricants in sexually active females as these products may alter normal vaginal and lower urethral flora.
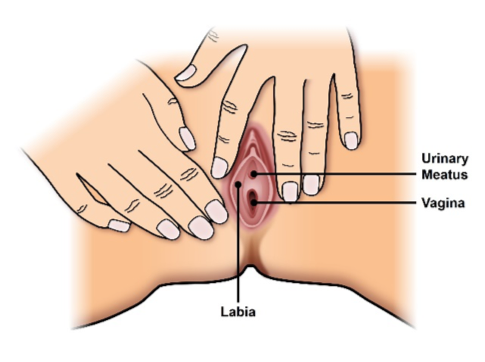
3. Assist the female patient in the identification of urinary meatus and anatomical position of the vagina in relation to the meatus. The use of a mirror, placed so that the patient can visualize perineal structures can be very helpful.
4. If postmenopausal female patient has hypoestrogenism perineal tissue, consider transvaginal estrogen medication.
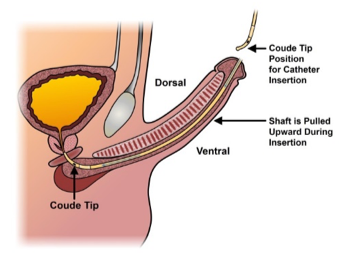
5. Teach male patients the correct positioning of the male urethra during insertion of the catheter to minimize trauma as the catheter passes through curved portions of the urethra.
6. Be careful to avoid touching the tip of the catheter and/or letting it touch other surfaces. In patients with recurrent catheter-associated infections, consider the use of a “no-touch” catheter or “no-touch” grip as seen in these pictures or that has a protective sleeve that the catheter is inserted through.

7. Use of a generous amount of lubricant along the length of the catheter (especially male patients) since dry catheters may cause excoriations in the urethra leading to an entry point for bacteria contamination.8. Keep bladder as empty as possible by having patients catheterize at least 4 to 6 times a day, approximately every four to six hours or to keep catheterized volume < 500 mLs. Keeping the bladder as empty as possible will prevent over-distension of the bladder and increases in intravesical pressure, all of which will preserve adequate blood supply to the bladder wall.
9. Encourage use of a new catheter each time performing IC. Most catheters are manufactured and packaged for single sterile use. Never reuse a hydrophilic catheter.
10. If the patient also has irritative bladder storage symptoms (e.g. urgency, frequency), consider prescribing an anticholinergic medication.
11. Drink adequate amount of water so that your urine is light yellow to yellow all day long. The color of urine can be a quick way to know whether you are drinking enough or too much during the day. If color gets dark or urine has a foul smell, increase water intake.
12. Acidification of the bladder may prevent bacteria growth. In the non-catheterizing populations, cranberry capsules and juice have been shown and recommended to help prevent the growth of bowel bacteria in the urethra and the bladder.
- Cranberry ingestion may be contra-indicated in some patients (e.g., those prone to oxalate or uric acid calculi). Cranberry is contraindicated in patients on anticoagulation therapy and should not be recommended to this group.
- Lactobacillus in the diet (yogurt) has been shown to prevent E.Coli from growing in the urethra. So taking a Probiotic tablet every day is recommended.
- Hiprex 1000mg combined with Vitamin C 1000 mg capsules twice times a day is thought to acidify urine enough to prevent bacterial growth in the bladder and is recommended in patients with recurrent UTIs.
Written by: Diane K. Newman, DNP, ANP-BC, FAAN, Adjunct Professor of Urology in Surgery, Perelman School of Medicine, University of Pennsylvania and Co-Director of the Penn Center for Continence and Pelvic Health
References:
1. Beauchemin L, Newman DK, Le Danseur M, Jackson A, Ritmiller M. Best practices for clean intermittent catheterization. Nursing. 48, 9 (Sept 2018):49-54.
2. Goetz LL, Droste L, Klausner AP, Newman DK. Catheters Used for Intermittent Catheterization. Clinical Application of Urologic Catheters, Devices and Products. Cham: Springer International Publishing; (2018):47-77.
3. Lamin E, & Newman DK. Clean intermittent catheterization revisited. Int Urol Nephrol. 48, 6 (Jun 2016): 931-9.
4. Newman DK, & Willson M. Review of intermittent catheterization and current best practices. Urologic Nursing. 31,1 (Jan-Feb 2011): 12-28, 48.