In our recent study,1 we aimed to address this gap by systematically assessing early perioperative morbidity after AUS implantation using the standardized complication reporting framework recommended by the European Association of Urology (EAU).2 To our knowledge, this represents the first study applying a predefined, procedure-specific complication catalog in accordance with these quality criteria in the context of AUS surgery.
We retrospectively evaluated 227 male patients undergoing AUS implantation at our institution (University Medical Center Hamburg-Eppendorf, Hamburg, Germany). Complications within the first six postoperative weeks were extracted using structured chart review and classified according to the Clavien–Dindo classification. Importantly, our predefined catalog included both major and minor adverse events to ensure comprehensive and transparent reporting.
We observed an overall complication rate of 47%, highlighting that early postoperative events are frequent. However, the majority of complications were minor and self-limiting. Bleeding complications, particularly hematomas, managed conservatively, represented the most common events. Major complications requiring surgical or radiologic intervention occurred in only 7.9% of cases and were predominantly related to urinary retention.
More than half of patients experienced no complications during the early postoperative period. The perceived morbidity of AUS implantation is highly dependent on the rigor of complication reporting. Minor events such as hematomas or bacteriuria are often underreported but may have clinical relevance, including potential impact on wound healing, infection risk, or long-term device survival. Without predefined reporting frameworks, these events are easily overlooked, leading to an underestimation of procedure-related morbidity and inconsistent interpretation of surgical outcomes.
Long-term device outcomes in our cohort were consistent with previously reported data. Over a median follow-up of more than four years, explantation was required in approximately one in five patients, most commonly due to urethral erosion and infection. These findings reflect the complexity of contemporary AUS patients, who are often older, multimorbid, and frequently have a history of pelvic radiotherapy or prior urethral surgery, factors known to increase the risk of adverse outcomes.
The clinical implications of our study are twofold: First, standardized complication reporting improves transparency and enables meaningful comparison across studies, centers, and surgical techniques. Second, it supports individualized patient counselling, which is particularly important given the elective nature of AUS implantation. Patients should be informed not only about long-term device durability but also about the realistic risk of early postoperative morbidity. Future research should focus on validating standardized reporting in multicenter cohorts and exploring the relationship between perioperative complications and patient-reported outcomes. Such efforts will help to refine risk stratification, optimize perioperative care, and ultimately improve shared decision-making.
In conclusion, AUS implantation remains a safe and effective treatment for male SUI, with frequent but predominantly minor perioperative complications. The application of standardized, procedure-specific complication reporting provides a more accurate and clinically meaningful understanding of surgical morbidity and should be adopted in future studies.
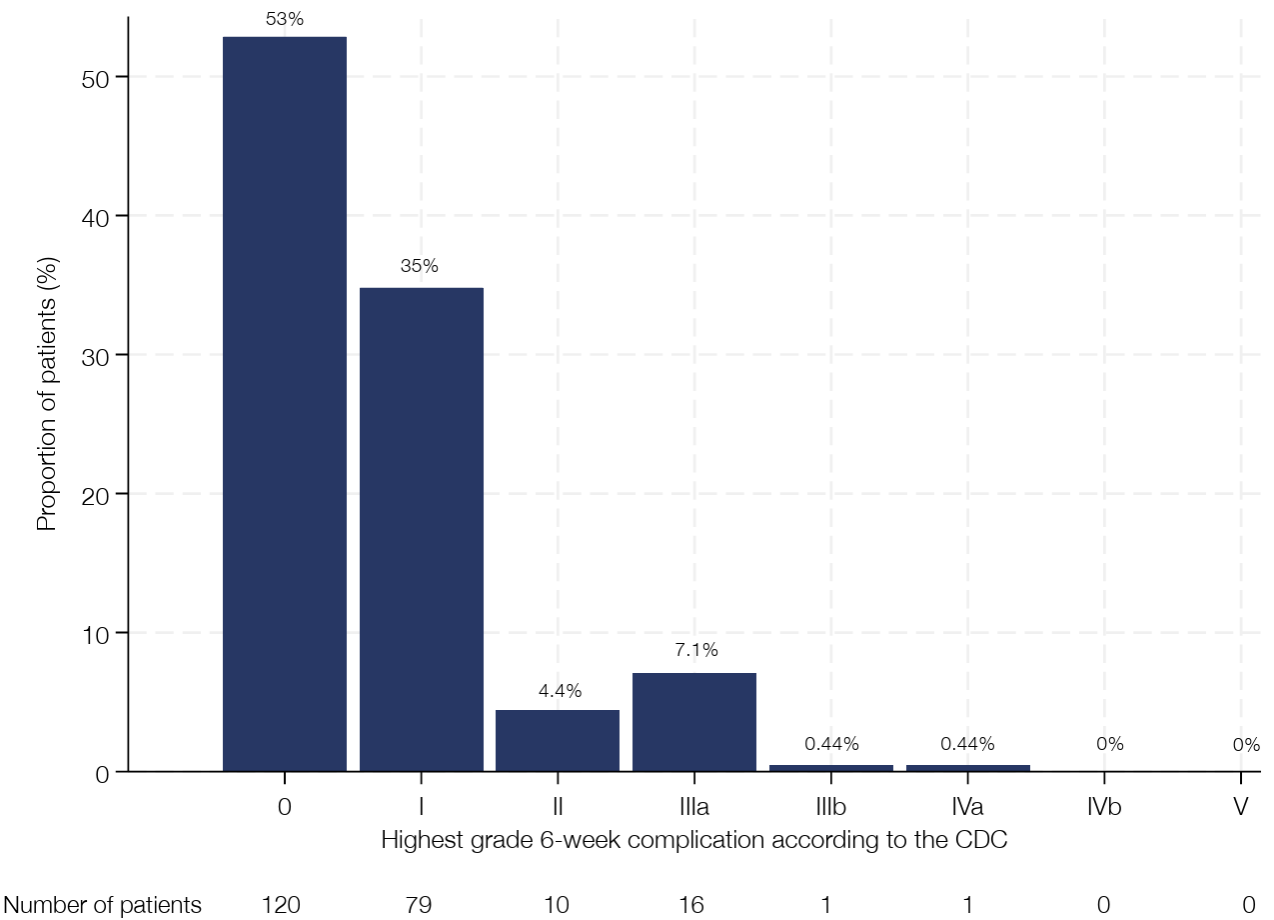
Figure 1 – Column chart depicting the distribution of the highest grade six-week complication per patient stratified by Clavien-Dindo classification.

Figure 2 – Kaplan–Meier curve illustrating explantation-free survival in 227 cases of artificial urinary sphincter implantation between 2015 and 2020. The curve is truncated at 72 months to minimize potential inaccuracies arising from the small number of patients remaining at risk beyond this time point.
Written by: Navid Roessler and Malte W. Vetterlein
Department of Urology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
References:
- Roessler N, Vetterlein MW, Konrad THJ, Schulz RJ, Wagner MC, Klemm J, Shariat SF, Dahlem R, Fisch M, Ludwig TA: Standardized reporting of perioperative complications after male artificial urinary sphincter implantation. World J Urol 2026, 44(1):156.
- Mitropoulos D, Artibani W, Graefen M, Remzi M, Rouprêt M, Truss M: Reporting and grading of complications after urologic surgical procedures: an ad hoc EAU guidelines panel assessment and recommendations. Eur Urol 2012, 61(2):341-349.