The data were extracted from the prospective, registered multicenter PROPEL study (ClinicalTrials.gov-Identifier: NCT00638235), in which 277 women with symptomatic 2.-4.stage cysto- or rectoceles with or without apical prolapse underwent vaginal mesh-supported vaginal sacrospinous ligament fixation using the Elevate system. From these women, 38 % (N=105) had anterior pain, 47 % (N=129) visceral, 44 % (N=122) posterior pain, while in total 68 % (N=187) suffered from any pelvic pain (table 1). The cure rates after 6 months of follow-up were for anterior pain 82.20 %, for visceral pain 85.25 %, and for posterior pain 58.77%.
Table 1 shows the prevalence of the different symptoms of overactive bladder and underactive bladder at baseline and 6 months postoperatively, with prevalences at baseline between 36.4% and 64.8% in the different pain subgroups. The cure rates (cure rate defined as disappearance of moderate or quite a bit symptom severity) at 6 months follow-up ranged between 64.7 % and 84.9 %.
Table 2 shows the prevalence of different symptoms of obstructive defecation and fecal incontinence, which varied at baseline between 8.0% and 51.4% in the different pain subgroups. The cure rates differed from 51.9% to 71.6%. All differences were, despite subgroups of PFDI 38, significant.
To understand these associations, we explain first the pathophysiology of symptom development (Figure 1). The main cause of POP is ligamentous connective tissue defects. In Figure 1, it is outlined that these defects, by different pathophysiologic pathways, can cause symptoms.
In women with POP, the apex and/or the anterior or posterior vaginal wall descend and are hypermobile. This can cause stretching of the nerve fibers of the plexus pelvicus, which contains sympathetic nerves from Th12 – L2 and parasympathetic nerves from S2-S4, also some somatic nerves from S2-S4. This stretching can cause pain. Lacerations of the nerve fibers can cause neuroinflammation, via axon reflexes, and pain in the peripheral tissues like vulva or bladder, can occur. Neuroinflammation can be associated with hypersensitivity. Due to the different affected nerve fibers, the pain location and character can differ and cause abdominal, visceral, and posterior pain.4,5 As shown, different urgency symptoms are often triggered by POP. According to the diagnostic algorithm,1 defect in all zones of the pelvic floor can be associated with symptoms of overactive bladder. Quaghebeur et al.6 described in detail that due to POP, the stretch receptors in the bladder base can be stimulated even in low bladder volumes, which will be felt as urinary urgency. Even a premature activation of the micturition reflex can occur, which can lead to urinary urgency incontinence.
The pelvic organs are fixated and suspended by ligaments and fascia, which hold them in their optimal position. The muscles of the pelvic floor – the levator plate (LP), pubococcygeus muscle (PCM), puborectalis muscle (PRM), and longitudinal muscle of the anus (LMA) – have important functions in the opening and closure of the urethra and anorectum.6,7 These muscles are striated and composed of sarcomeres for which a relationship between muscle force and muscle length exists.8 Only in a small range of length, optimal muscle force is available (Figure 2). As in women with POP, the insertion areas of these muscles are dislocated, and the muscles can be lengthened, which leads to immediate loss of muscle force (see Figure 2). Repositioning of the vaginal wall can restore muscle length and, therefore, force and function.
This mechanism is important in understanding abnormal micturition in women with POP. Normal micturition is only possible by active opening of the proximal urethra by the posteriorly located muscles LP and LMA. This is necessary/essential because, due to Hagen-Poiseuille`s law, the resistance to flow is inversely proportional to the radius (4th power). So, with a closed urethra, at least 100-fold bladder pressure would be necessary to start micturition,9,10 if this active opening from the outside would not be performed. If in women with POP, the posterior muscles LP and LMA lengthen, the opening forces can be reduced. Obstructive micturition occurs, resulting in trabeculation of the detrusor, symptoms of abnormal emptying, and possible residual volume after micturition. The flow through the urethra is proportional to the radius in 4th power. For instance, a reduction of the radius by half results in a reduction of the flow to 1/16.
For fecal continence, the optimal forming of the anorectal angle is important, with LP pulling backwards and PRM pulling forwards. Reduction of muscle forces in POP can cause fecal incontinence, while repairing the POP muscle length, force, and function restores. How rectoceles and apical prolapse can cause obstructive defecation is explained in Gold et al.7
Summary:
Meanwhile, we know the main mechanisms in the development of POP due to ligamentous defects. The same defects are responsible – via known pathophysiological pathways – for the development of pain, symptoms of over- and underactive bladder, and anorectal dysfunction. So, the coexistence of POP and all of these symptoms can be explained by these mechanisms. Pain symptoms, which are present in up to 67 % in women with symptomatic POP, can be cured in high percentages by mesh-supported vaginal sacrospinous ligament fixation. We were able to show that coexistent bladder and bowel symptoms can be cured in high percentages.
This has important implications: Urologists should learn to detect POP as a cause of overactive and underactive bladder, anorectal dysfunctions, and pelvic pain, and advise on possible long-lasting cure by surgery. Especially in women with pelvic pain and urinary urgency symptoms, POP should be excluded as a differential diagnosis before the diagnosis of interstitial cystitis/bladder pain syndrome is established.
Table 1 Coexisting Urinary Symptoms in Women with Pelvic Organ Prolapse and Pelvic Pain (with permission from (3) and (11)).

Prevalences (expressed as relative frequencies) of overactive-bladder and underactive-bladder symptoms of R2 severity (moderate or quite a bit of complaints) pre- and 6 months postoperatively in the groups of patients with anterior, visceral, posterior, or total pain at baseline.
Additionally, the symptom cure rates (disappearance of moderate and quite a few symptoms) and the p-values of the conducted McNemar-tests using to compare the prevalence-rates between baseline and 6 months up period are depicted. The inferential comparisons imply the formulation and testing of two hypotheses like these: Ho: P (rel. frq. to NB) ≤ P(rel.frq. to N6m) vs. H1: P(rel.frq. to NB) > P(rel.frq. to N6m).11
Table 2 Coexisting Bowel Symptoms in Women with Pelvic Organ Prolapse and Pelvic Pain (with permission from (3) and (11)).

Prevalences (expressed as relative frequencies) of fecal-incontinence and obstructive-defecation R2-symptoms (moderate or quite a bit severity) pre and 6 months post surgery in the groups of patients with anterior, visceral, posterior, or total pain at baseline.
Additionally, the relative ratios, the symptom cure rates (disappearance of moderate and quite a bit symptom), and the p-values of the conducted McNemar-tests used to compare the prevalence-rates between baseline and 6 months up period are depicted. The inferential comparisons imply the formulation and testing of two hypotheses like these: Ho: P (rel. frq. to NB) ≤ P(rel.frq. to N6m) vs. H1: P(rel.frq. to NB) > P(rel.frq. to N6m).
Main cause: laxity/looseness of connective tissue/supporting ligaments of pelvic floor
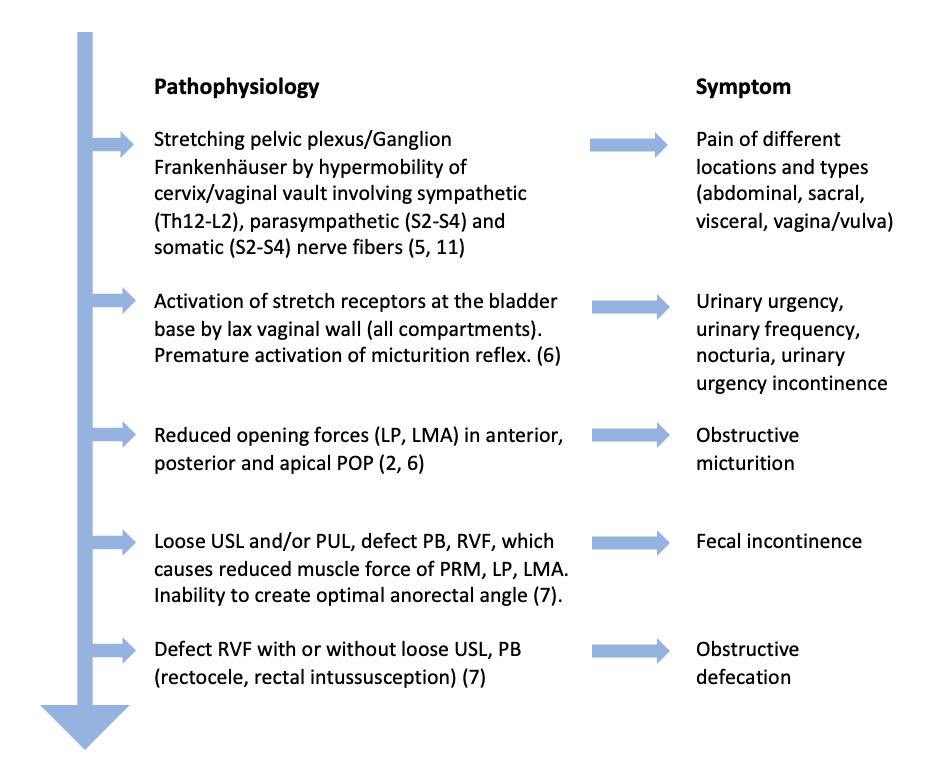
Figure 1 Co-Existence of pelvic organ prolapse and different symptoms: etiology and pathophysiologic pathways. LP: levator plate; LMA: longitudinal muscle of anus; USL: uterosacral ligament; PUL: pubourethral ligament; PRM: puborectalis muscle; RVF: rectovaginal fascia; PB: perineal body; POP: pelvic organ prolapse:
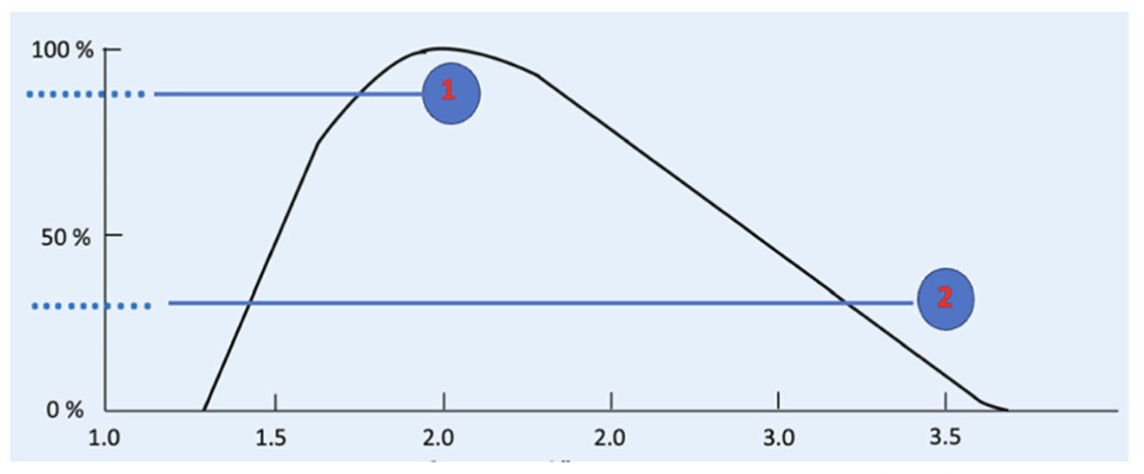
Figure 2: In a non-descended vaginal wall, a muscle fiber of LP, LMA, PCM, or PRM (see Figure 1) can have normal length (1) with maximal muscle force. If in women the vaginal wall descends in POP, the muscle fiber can lengthen to position 2 with immediate loss of muscle force. Reposition of the descended vaginal wall enables recovery of the muscle force.
Written by: Lena Schmidbauer,1 Bernhard Liedl,1 Maren Juliane Wenk2
- Urologische Klinik München-Planegg, Germany
- Klinik für Urologie und Urochirurgie, Universitätsmedizin Mannheim, Germany
- Liedl B, Dodi G, Inoue H, Neuman M, del Amo E. Structural, functional, and dysfunctional pelvic anatomy. 2024.
- Liedl B, Barba M, Wenk M. Pelvic Floor Reconstruction-Update 2024: Prolapse-Associated Symptoms and Their Treatment - Beyond the Abstract. Urotoday. 2024.
- Schmidbauer L, Liedl B, Goeschen K, Antoniewicz A, Kurtzman J, Wenk MJ. Coexistence of Pelvic Pain, Bladder, and Bowel Symptoms in Women with Pelvic Organ Prolapse: The Effect of Transvaginal Surgery. International Urogynecology Journal. 2025.
- Petros PEP. Chronic Pelvic Pain of Unknown Origin: Considerations on Uterosacral Ligament Pathogenesis and Cure. BJOG. 2025.
- Liedl B, Goeschen K, Grigoryan N, Sutherland SE, Yassouridis A, Witczak M, et al. The Association Between Pelvic Organ Prolapse, Pelvic Pain and Pelvic Reconstructive Surgery Using Transvaginal Mesh: A Secondary Analysis of a Prospective Multicenter Observational Cohort Trial. Journal of Clinical Gynecology and Obstetrics. 2020;9(4):79-95.
- Quaghebeur J, Bush M, Shkarupa D, Wyndaele JJ, De Wachter S. A brief physiology and pathophysiology of the bladder. Ann Transl Med. 2024;12(2):24.
- Gold DM, Swash M, Farag A, Ding S, Santoro G, Dodi G. A brief physiology and pathophysiology of the anorectum based on the Integral Theory paradigm. Ann Transl Med. 2024;12(2):25.
- Gordon AM, Huxley AF, Julian FJ. The variation in isometric tension with sarcomere length in vertebrate muscle fibres. J Physiol. 1966;184:170-92.
- Bush MB, Liedl B, Wagenlehner F, Petros P. A finite element model validates an external mechanism for opening the urethral tube prior to micturition in the female. World J Urol. 2015;33(8):1151-7.
- Wenk MJ, Bush M, Swash M, Liedl B, Witczak M. Underactive bladder, Fowler's syndrome are potentially curable by uterosacral ligament repair. Ann Transl Med. 2024;12(2):34.
- Schmidbauer L. Urinary Urgency and Chronic Pelvic Pain in Women with Pelvic Organ Prolapse (POP) vs. Bladder Pain Syndrome/Interstitial Cystitis (BPS/IC): LMU München; 2026.