The urologic component begins with suprapubic (SP) tube insertion and vaginectomy (Fig 1).
Fig 1: Vaginectomy. Mucosa is sharply excised and cauterized.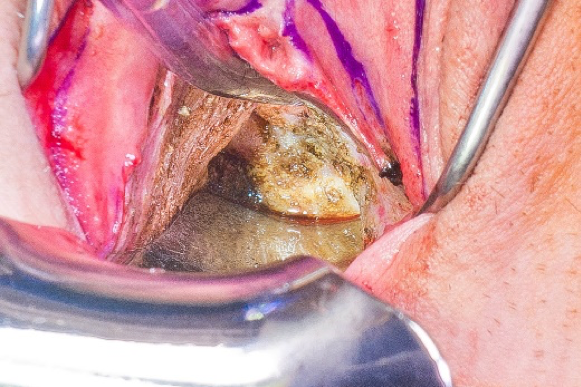
The labia minora is marked and local flaps are created around the native urethral meatus for pars fixa urethroplasty. Patients with a large clitoris and plentiful labia minora tissue undergo U-shaped urethroplasty (Fig 2).
Fig 2. U-shaped pars fixa urethroplasty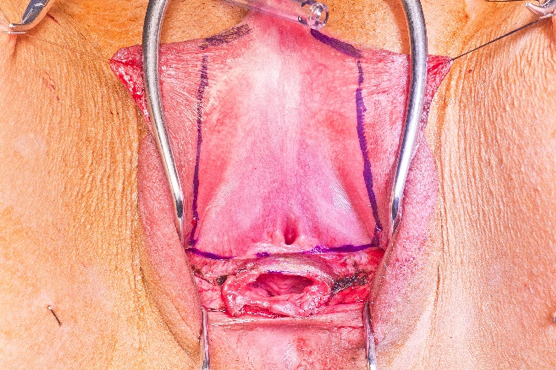
Patients with smaller clitorises with deficient labia minora may benefit from a ring flap urethroplasty (Fig 3). This allows tension-free translocation of the distal PF urethral meatus to the mons pubis. The periurethral fornices are also de-epithelialized to allow for cylindrical urethral reconstruction with resultant standard urethral catheter insertion.
Fig 3A. Ring Flap Markings. Labia minora tissue flanking the vaginal introitus is included in the urethroplasty.
Fig 3B. Ring Flap dissection. The periurethral fornices are de-epithelialized. The ring is transected in the midline and bilateral labia minora flaps are demarcated. 
Fig 3C. Labia minora flap elevation with chordee release.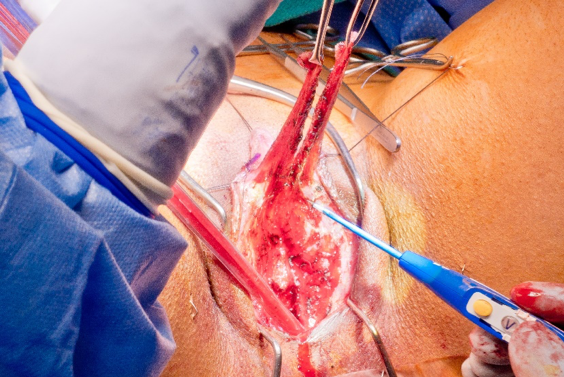
Fig 3D. Labia minora flap pars fixa urethroplasty, dorsal closure.
Fig 3E. Ring Flap urethroplasty ventral closure.
To support the proximal PF urethroplasty suture line, vascularized flaps proximal to the labia minora flaps are developed (Fig 4).
Fig 4A. Flaps for native urethral meatus to PF urethral anastomotic suture line coverage are lateral to the urethral meatus.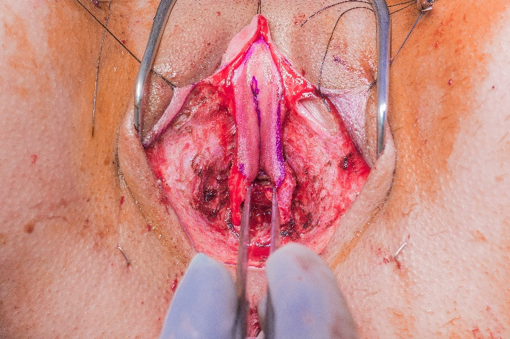
Fig 4B. Flaps directly cover the native urethral meatus to proximal PF urethra suture line after ventral closure of the PF urethra.
The clitoris is subsequently de-epithelialized and the suspensory ligament transected. We then isolate one of the dorsal nerve bundles, which is identified between the corpora cavernosa and Buck’s fascia (Fig 5).
Fig 5. Dorsal nerve isolated.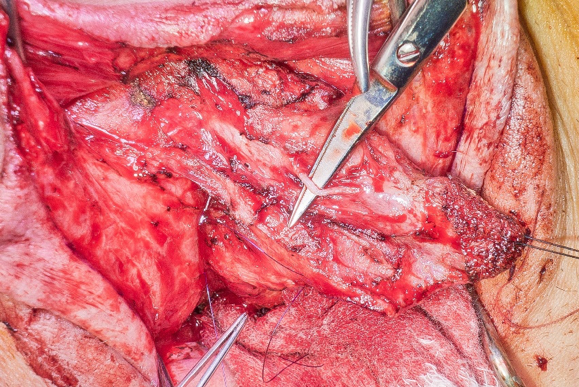
An opening is then made overlying the pubic symphysis, and the distal PF urethra and de-epithelialized clitoris are translocated to the infra pubic position (Fig 6). The urethral catheter is then inserted to facilitate perineal reconstruction.
Fig 6. Translocation of distal urethra and clitoris.
Labia majora rotational advancement flaps are subsequently developed to create an anteriorly positioned pouch-like scrotum (Fig 7).
Fig 7A. Scrotoplasty labia majora flap development.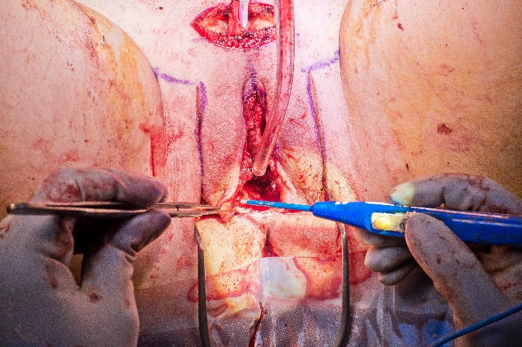
Fig 7B. Scrotoplasty labia majora flaps elevated.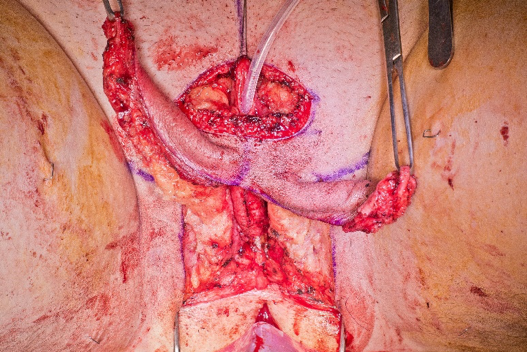
Fig 7C. Scrotoplasty labia majora flaps advanced and rotated to create pouchlike 
Fig 7D. Scrotoplasty completed with inset RF Phallus with no glans.
Perineal reconstruction involves multi-layered closure, with the first layer covering the PF urethral suture line (Fig 8).
Fig 8A. Perineal reconstruction begins with closure of the bulbospongiosus layer over the PF urethral suture line.
Fig 8B. Perineal reconstruction complete. An inverted Y closure of the perineum decreases the occurrence of a perineal divot.
As the reconstructive urologist completes the genital masculinization of the perineum, the microsurgical team harvests the radial forearm (RF) free flap or anterolateral thigh (ALT) pedicled (or free) flap and fashions it into the neophallus and pars pendulans urethra (Fig 9).
Fig 9A. Radial Forearm flap has been elevated and the urethral and phallus component separated by a de-epithelialized segment.
Fig 9B. Phallus component of the flap has been wrapped around the urethra, and the glansplasty with meatoplasty have been completed.
Concomitant glansplasties are performed in many RF neophalluses. Occasionally, the RF glansplasty is delayed if the flap is excessively thin. Glansplasty is delayed in ALT neophalluses due to a higher risk of distal flap necrosis.
In RF phalloplasty, the microsurgeons will subsequently make an incision in the groin to expose the femoral vessels. The flap vessels are then divided and the neophallus is brought towards the midline infra pubic position. The urologist performs the urethral anastomosis (Fig 10).
Fig 10. PF-PP anastomotic urethroplasty.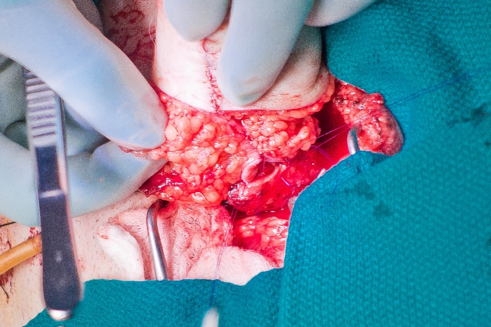
Utilizing an operative microscope, the microsurgeons complete the coaptation between the dorsal nerve and lateral antebrachial or lateral femoral cutaneous nerve followed by the vascular anastomoses of the flap. The neophallus is then fully inset and the wounds are closed (Fig 11).
Fig 11A. RF Phallus completely inset.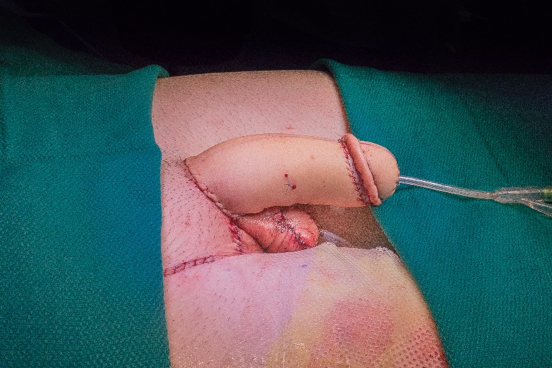
Fig 11B. RF Phallus completely inset.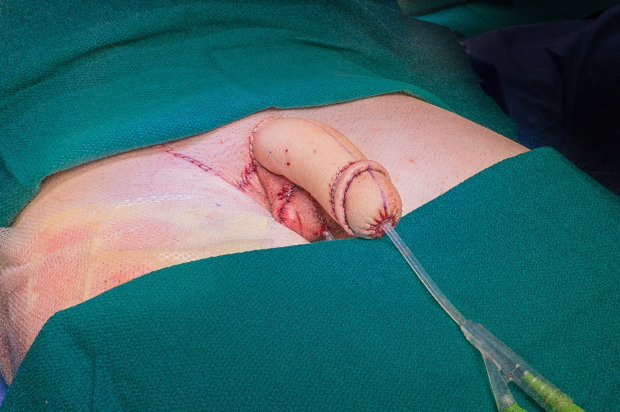
The donor site is covered with thick split thickness sheet grafts (STSG) harvested from the thigh (Fig 12).
Fig 12. Donor site closure with STSG.
Approximately 1 year after phalloplasty, most patients will have erotic and tactile sensation in their neophallus and many will seek prosthetic surgery to achieve penetrative sexual function. Penile implants inserted are malleable or inflatable (Fig 13).
Fig 13. Penile implant insertion after phalloplasty.
Male genital aesthetics and urinary function can be achieved in a single stage via phalloplasty with urethroplasty, vaginectomy, scrotoplasty, and perineal reconstruction. Sexual function via prosthetic surgery is offered after patients develop protective tactile sensation in their neophallus and are voiding reliably. Patients with urethral complications require repair prior to the insertion of implants.
Written by: Mang L. Chen, MD, and Bauback Safa, MD, MBA, California Pacific Medical Center, San Francisco, California, USA.
Read the Abstract