In terms of physiology, testosterone actually appears to be beneficial for the prevention of LUTS/BPH.1,2 Studies have suggested three major contributors to LUTS/BPH: nitric oxide deficiency, autonomic hypertonicity, and pelvic atherosclerosis. Among other things, these entities result in pelvic ischemia and chronic hypoxia of the bladder and prostate, which has been associated with LUTS/BPH.3-6 Sharing a similar pathway with phosphodiesterase-5 (PDE-5) inhibitors, testosterone has been shown to alleviate this hypoxia by modulating cGMP-mediated nitric oxide production.7-10
The notion of prostatic growth being proportional to testosterone levels likely stems from the sentinel papers of Huggins et al in the 1940s, in which castration resulted in prostate cancer regression and T administration caused prostate growth.11 Of note, this landmark study was comprised of only one patient, and involved prostate cancer rather than normal prostatic tissue, which may have influenced the results. More recent evidence suggests a saturation model to prostatic growth, with androgen receptors becoming saturated at near castrate levels.12 This makes sense given that prostate volume has been shown to increase with time regardless of testosterone levels. As such, men continue to have prostate growth despite waning bioavailable T with age, and young men do not see a spike in prostatic growth with high T levels seen in early adulthood (Figure 1). It is also worth noting that increasing prostate size does not correlate with worsening LUTS/BPH, as has been shown by numerous studies.13,14 Thus the antiquated idea of testosterone fueling prostatic growth still should have no bearing on urinary symptoms.
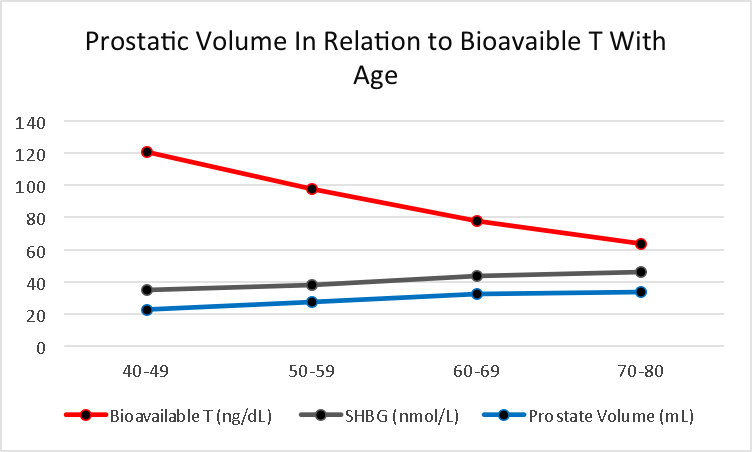
Figure 1: Graph of bioavailable T, SHBG, and prostate volume with age. Note increasing prostatic volume increase despite lowering levels of bioavailable T.
Graph created with raw data from St. Sauver et al and Muller et al.
Finally, to date there are multiple studies that have shown there to be no relationship between TRT and worsening LUTS/BPH. On the contrary, some studies have suggested improvements of LUTS with TRT, likely through the mechanisms mentioned above. It is the authors’ opinion that TRT is not a risk factor for LUTS/BPH and the warning set forth by the FDA likely needs reevaluation.
Written by: Wesley Baas and Tobias S. Köhler, Division of Urology, Southern Illinois University School of Medicine, Springfield, IL, USA.
Read the Abstract
References:
1. Saad F, Gooren L, Haider A, Yassin A. An exploratory study of the effects of 12 month administration of the novel long-acting testosterone undecanoate on measures of sexual function and the metabolic syndrome. Archives of andrology 2007;53:353-7.
2. Yassin DJ, Doros G, Hammerer PG, Yassin AA. Long-term testosterone treatment in elderly men with hypogonadism and erectile dysfunction reduces obesity parameters and improves metabolic syndrome and health-related quality of life. The journal of sexual medicine 2014;11:1567-76.
3. Bloch W, Klotz T, Loch C, Schmidt G, Engelmann U, Addicks K. Distribution of nitric oxide synthase implies a regulation of circulation, smooth muscle tone, and secretory function in the human prostate by nitric oxide. The Prostate 1997;33:1-8.
4. Mitterberger M, Pallwein L, Gradl J, et al. Persistent detrusor overactivity after transurethral resection of the prostate is associated with reduced perfusion of the urinary bladder. BJU international 2007;99:831-5.
5. Tarcan T, Azadzoi KM, Siroky MB, Goldstein I, Krane RJ. Age-related erectile and voiding dysfunction: the role of arterial insufficiency. British journal of urology 1998;82 Suppl 1:26-33.
6. Zhao C, Kim SH, Lee SW, et al. Activity of phosphodiesterase type 5 inhibitors in patients with lower urinary tract symptoms due to benign prostatic hyperplasia. BJU international 2011;107:1943-7.
7. Gacci M, Corona G, Salvi M, et al. A systematic review and meta-analysis on the use of phosphodiesterase 5 inhibitors alone or in combination with alpha-blockers for lower urinary tract symptoms due to benign prostatic hyperplasia. European urology 2012;61:994-1003.
8. McVary KT, Roehrborn CG, Kaminetsky JC, et al. Tadalafil relieves lower urinary tract symptoms secondary to benign prostatic hyperplasia. The Journal of urology 2007;177:1401-7.
9. Shigehara K, Namiki M. Late-onset hypogonadism syndrome and lower urinary tract symptoms. Korean journal of urology 2011;52:657-63.
10. Stief CG, Porst H, Neuser D, Beneke M, Ulbrich E. A randomised, placebo-controlled study to assess the efficacy of twice-daily vardenafil in the treatment of lower urinary tract symptoms secondary to benign prostatic hyperplasia. European urology 2008;53:1236-44.
11. Huggins C, Hodges CV. Studies on prostatic cancer: I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. The Journal of urology 2002;167:948-51.
12. Morgentaler A, Traish AM. Shifting the paradigm of testosterone and prostate cancer: the saturation model and the limits of androgen-dependent growth. European urology 2009;55:310-20.
13. Barry MJ, Cockett AT, Holtgrewe HL, McConnell JD, Sihelnik SA, Winfield HN. Relationship of symptoms of prostatism to commonly used physiological and anatomical measures of the severity of benign prostatic hyperplasia. The Journal of urology 1993;150:351-8.
14. Castro JE, Griffiths HJ, Shackman R. Significance of signs and symptoms in benign prostatic hypertrophy. British medical journal 1969;2:598-601.
Finally, to date there are multiple studies that have shown there to be no relationship between TRT and worsening LUTS/BPH. On the contrary, some studies have suggested improvements of LUTS with TRT, likely through the mechanisms mentioned above. It is the authors’ opinion that TRT is not a risk factor for LUTS/BPH and the warning set forth by the FDA likely needs reevaluation.
Written by: Wesley Baas and Tobias S. Köhler, Division of Urology, Southern Illinois University School of Medicine, Springfield, IL, USA.
Read the Abstract
References:
1. Saad F, Gooren L, Haider A, Yassin A. An exploratory study of the effects of 12 month administration of the novel long-acting testosterone undecanoate on measures of sexual function and the metabolic syndrome. Archives of andrology 2007;53:353-7.
2. Yassin DJ, Doros G, Hammerer PG, Yassin AA. Long-term testosterone treatment in elderly men with hypogonadism and erectile dysfunction reduces obesity parameters and improves metabolic syndrome and health-related quality of life. The journal of sexual medicine 2014;11:1567-76.
3. Bloch W, Klotz T, Loch C, Schmidt G, Engelmann U, Addicks K. Distribution of nitric oxide synthase implies a regulation of circulation, smooth muscle tone, and secretory function in the human prostate by nitric oxide. The Prostate 1997;33:1-8.
4. Mitterberger M, Pallwein L, Gradl J, et al. Persistent detrusor overactivity after transurethral resection of the prostate is associated with reduced perfusion of the urinary bladder. BJU international 2007;99:831-5.
5. Tarcan T, Azadzoi KM, Siroky MB, Goldstein I, Krane RJ. Age-related erectile and voiding dysfunction: the role of arterial insufficiency. British journal of urology 1998;82 Suppl 1:26-33.
6. Zhao C, Kim SH, Lee SW, et al. Activity of phosphodiesterase type 5 inhibitors in patients with lower urinary tract symptoms due to benign prostatic hyperplasia. BJU international 2011;107:1943-7.
7. Gacci M, Corona G, Salvi M, et al. A systematic review and meta-analysis on the use of phosphodiesterase 5 inhibitors alone or in combination with alpha-blockers for lower urinary tract symptoms due to benign prostatic hyperplasia. European urology 2012;61:994-1003.
8. McVary KT, Roehrborn CG, Kaminetsky JC, et al. Tadalafil relieves lower urinary tract symptoms secondary to benign prostatic hyperplasia. The Journal of urology 2007;177:1401-7.
9. Shigehara K, Namiki M. Late-onset hypogonadism syndrome and lower urinary tract symptoms. Korean journal of urology 2011;52:657-63.
10. Stief CG, Porst H, Neuser D, Beneke M, Ulbrich E. A randomised, placebo-controlled study to assess the efficacy of twice-daily vardenafil in the treatment of lower urinary tract symptoms secondary to benign prostatic hyperplasia. European urology 2008;53:1236-44.
11. Huggins C, Hodges CV. Studies on prostatic cancer: I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. The Journal of urology 2002;167:948-51.
12. Morgentaler A, Traish AM. Shifting the paradigm of testosterone and prostate cancer: the saturation model and the limits of androgen-dependent growth. European urology 2009;55:310-20.
13. Barry MJ, Cockett AT, Holtgrewe HL, McConnell JD, Sihelnik SA, Winfield HN. Relationship of symptoms of prostatism to commonly used physiological and anatomical measures of the severity of benign prostatic hyperplasia. The Journal of urology 1993;150:351-8.
14. Castro JE, Griffiths HJ, Shackman R. Significance of signs and symptoms in benign prostatic hypertrophy. British medical journal 1969;2:598-601.