The clinical challenge is that these skills are traditionally acquired in the operating room through supervised “on-the-job” exposure. However, modern surgical education increasingly recognizes that the operating room should not be the first place where a trainee encounters the basic technical challenges of a procedure. Patient safety, reduced working hours, limited operative exposure, and the need for standardized assessment have all increased the importance of simulation-based surgical training. This is particularly relevant in transurethral surgery, where errors in orientation, loop control, or resection depth may lead to bleeding, capsular perforation, bladder perforation, incomplete resection, or inadequate sampling.
Simulation offers a risk-free environment where trainees can repeat key procedural steps, make mistakes without harming patients, and gradually acquire confidence before moving to supervised clinical practice. However, not every simulator is automatically useful simply because it resembles an organ or allows an instrument to be inserted. Before a model can be integrated into a structured curriculum, it needs to be evaluated carefully. This was the main motivation behind our study.
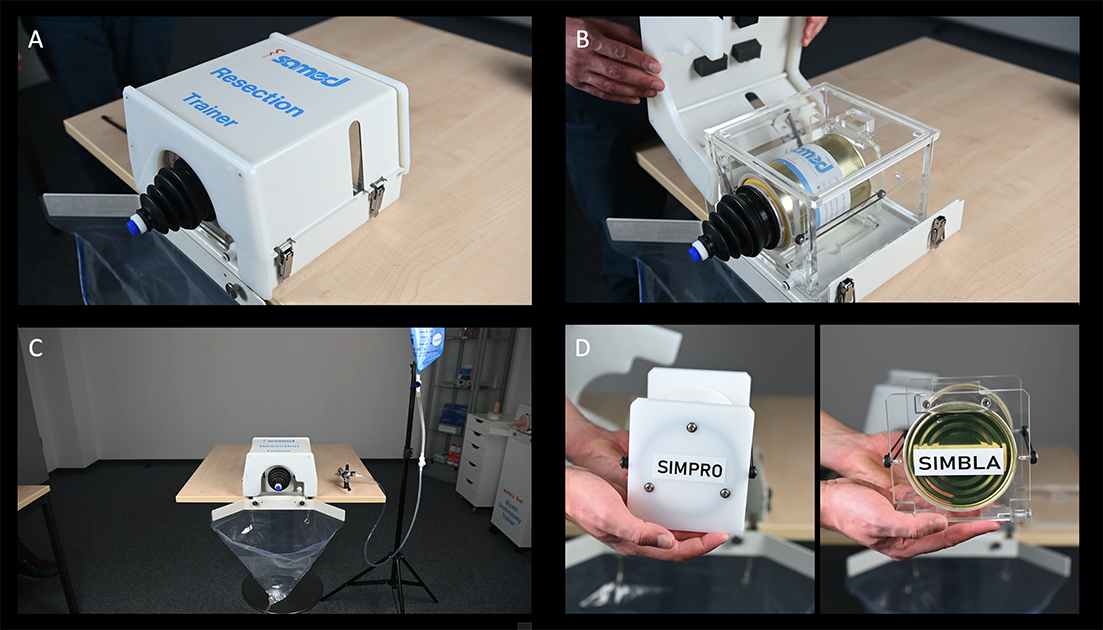
In our recently published article, we evaluated two bench-top simulation models designed for TURP and TURB training. The study was conducted within the framework of the European School of Urology and the EAU Lower Urinary Tract Endoscopy Working Group. Fourteen expert endourologists from multiple European centers assessed the models during EUREP 2025. In this study, experts were defined as consultant urologists with experience of more than 200 TURP and TURB procedures, ensuring that the evaluation reflected the perspective of surgeons clearly beyond the learning curve.
The evaluation focused on face validity and content validity. Face validity refers to whether experts perceive the model as realistic and useful for training. Content validity examines whether the model adequately covers the essential components of the procedure. These two forms of validation are important early steps before a simulator can be considered for broader curriculum integration.
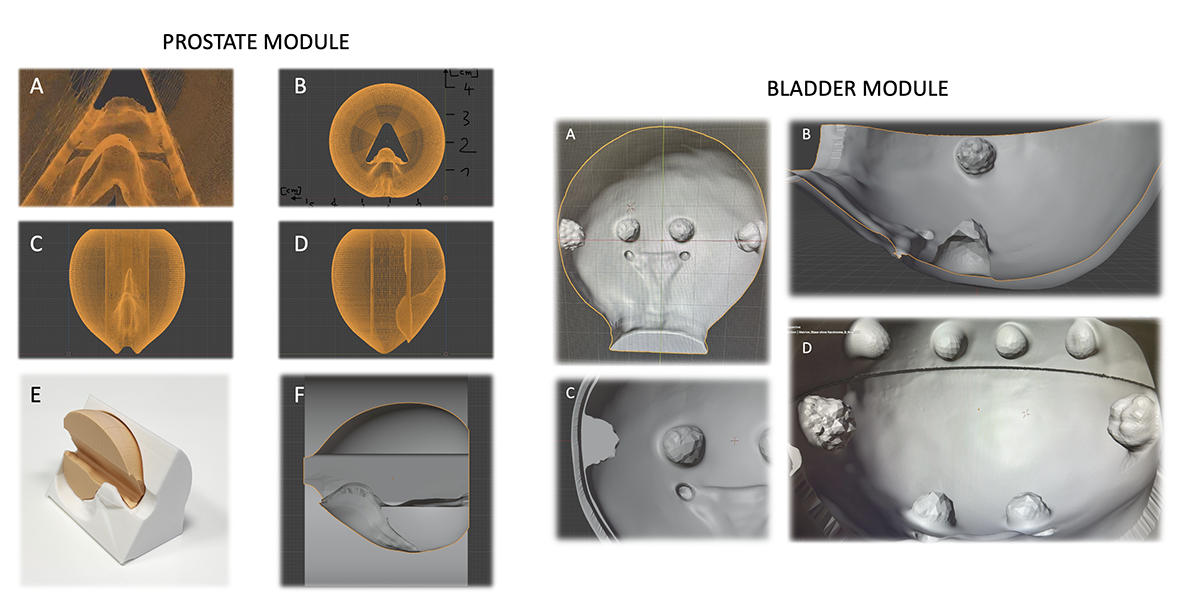
The most important message of our study is that both models were considered valuable for teaching core procedural skills. For TURP, experts rated the simulator highly for resectoscope handling, ergonomics, anatomical orientation, loop control, resection of median and lateral lobes, chip evacuation, and assessment of completeness of resection. For TURB, the model was rated favorably for cystoscope and resectoscope orientation, tumor identification, loop movement, resection depth, tumor base sampling, tissue fragment retrieval, and completeness assessment.
A key aspect of our analysis was the distinction between what the simulators were designed to teach and what they were not designed to reproduce. This distinction is important in surgical simulation. A bench-top simulator may be very effective for teaching hand-eye coordination, instrument orientation, loop control, resection sequence, and depth awareness, but may not reproduce bleeding, obturator reflex, or energy modulation. If these non-modeled features are included in the overall score without interpretation, the educational value of the simulator may be underestimated.
For this reason, we reported both the conventional scale-level content validity index and an adjusted analysis focused on core procedural skills. The results indicated strong expert consensus regarding the relevance for essential training objectives. Our findings suggest that the models are particularly suitable for early-stage skill acquisition and structured repetitive practice.
The limitations of these models are equally important to acknowledge. Neither simulator currently reproduces important intraoperative events such as bleeding or the obturator reflex. They also do not fully simulate energy modulation or the complexity of real-time complication management. Therefore, these models should not be presented as complete replacements for operating-room training. Rather, they should be understood as one component of a broader educational pathway.
Hands-on training is particularly important because each endoscopic procedure has its own technical language, anatomical landmarks, and risk points. A trainee who is generally familiar with endoscopic instruments may still be unprepared for the specific demands of TURP or TURB. In TURP, the surgeon must understand the relationship between the verumontanum, bladder neck, lateral lobes, median lobe, surgical capsule, and external sphincter while maintaining controlled loop movement and depth awareness. In TURB, the operator must identify tumor location, orient the resectoscope within the bladder, control the depth of resection, retrieve tissue fragments, and obtain an adequate tumor base sample while avoiding perforation or injury to critical structures. These are not abstract concepts; they are procedure-specific psychomotor and cognitive skills that need to be rehearsed before the trainee performs them on a patient.
This is where hands-on simulation has a unique educational value. It allows the trainee to repeat the same procedural steps in a standardized environment, receive immediate feedback, and gradually develop the visual-spatial orientation and instrument control required for safe surgery. Repetition is especially important in transurethral procedures, where small errors in loop movement, depth perception, or orientation may have relevant clinical consequences. A structured hands-on model gives the trainee the opportunity to make and correct these errors before entering the operating room.
In this sense, the value of a simulator should not be judged only by whether it reproduces every intraoperative event. Its educational value also lies in whether it prepares the trainee for a specific surgery by allowing deliberate practice of the core steps of that operation. The models evaluated in our study were particularly strong in this regard: experts considered them useful for anatomical orientation, resectoscope handling, loop control, resection depth, chip evacuation, and completeness assessment, which are central components of safe TURP and TURB performance.
This point is central to our view of simulation-based education. A simulator is not a curriculum by itself, and a hands-on course is not simply a demonstration of a device. The educational goal should be safe, stepwise preparation for a defined surgical procedure. Simulation becomes meaningful when it is integrated into a structured training program with defined learning objectives, progressive difficulty, expert feedback, objective assessment tools, and ultimately supervised transfer to clinical practice. In this context, the TURP and TURB models evaluated in our study may serve as practical tools for the early phases of transurethral surgery training.
The modular and reproducible nature of the simulators is also important. Biological models may offer tactile realism, but they can be difficult to standardize, store, reproduce, and use repeatedly across multiple training centers. Virtual reality platforms can provide metrics and simulate some dynamic events such as bleeding, but they may be expensive or limited in haptic realism. Bench-top modular models occupy a useful middle ground: they are clean, repeatable, relatively simple to implement, and suitable for hands-on courses and curriculum-based training.
Looking ahead, the ideal training pathway may involve a hybrid approach. Physical bench-top models may be best suited for early anatomical orientation, instrument handling, loop control, and tissue resection practice. More advanced virtual reality or augmented platforms may then be used to expose trainees to dynamic intraoperative scenarios such as bleeding, hemostasis, obturator reflex, or complication management. In this way, different simulation tools should not be viewed as competitors, but as complementary components of a progressive training pathway.
Another important implication of this study is assessment. In surgical education, the goal is not only to provide practice but also to define when a trainee is ready to progress. A validated model can help create objective assessment stations where trainees are evaluated on specific components such as orientation, loop control, resection depth, efficiency, safety, and completeness. This is particularly relevant for organizations such as the European School of Urology, where structured, stepwise, and competency-based training pathways are being developed.
Our findings should therefore be interpreted as an early but important step. The present study established face and content validity from expert endourologists. The next steps should include construct validity studies to determine whether the models can differentiate between novice, intermediate, and expert performance. Future work should also evaluate trainee learning curves, educational impact, and transfer of skills from the simulation environment to the operating room.
In summary, our study supports the role of TURP and TURB bench-top simulators as valuable tools for structured endourological training. They cannot reproduce every aspect of real surgery, and they should not be expected to do so. Their strength lies in providing a standardized, safe, and repeatable platform for learning the fundamental technical steps of transurethral resection. When used appropriately within a broader curriculum, these models may help improve the way we teach, assess, and ultimately perform endoscopic urological surgery.
Written by: Tarik Emre Sener, MD, FEBU, Department of Urology, School of Medicine, Marmara University, Istanbul, Türkiye
On behalf of the EAU European School of Urology (ESU) Lower Urinary Tract Endoscopy Working Group
Read the Abstract