Among thermally based techniques, Rezum employs convective water vapor to ablate prostatic tissue. It can be performed under local anesthesia, typically as a short outpatient procedure, and yields durable improvements in IPSS, QoL, and Qmax up to 5 years. Its low retreatment rate and preservation of erectile and ejaculatory function make it an excellent option for men seeking effective, minimally invasive symptom relief. CoreTherm transurethral microwave thermotherapy (TUMT) represents another thermal option with over two decades of clinical experience. It provides meaningful functional improvements and remains particularly valuable for patients with larger glands or those in urinary retention, unfit for surgery. However, this modality also shows the highest surgical retreatment rate among MISTs, reaching up to 23% at 5 years according to the current literature.
Mechanical interventions offer a distinct mechanism of action. The iTind device temporarily reshapes the prostatic urethra over 5-7 days without leaving an implant. It provides rapid and sustained improvement in LUTS, with durability beyond four years and preservation of sexual function. The UroLift system, in contrast, uses permanent implants to retract obstructive tissue. Long-term data demonstrate durable efficacy with a 5-year surgical retreatment rate of around 13%.
Other modalities introduce novel mechanisms. Optilume BPH, a drug-coated balloon dilation system, combines mechanical decompression with localized paclitaxel delivery to inhibit hyperplastic regrowth. Results from the randomized PINNACLE and long-term EVEREST trials confirm durable efficacy and near-complete preservation of erectile and ejaculatory function over four years. Similarly, transperineal laser ablation (TPLA), also known as Echolaser, enables precise, ultrasound-guided coagulative necrosis of the prostate through a transperineal approach. It is performed under local anesthesia and preserves sexual function in most men while providing substantial improvements in LUTS and flow rates.
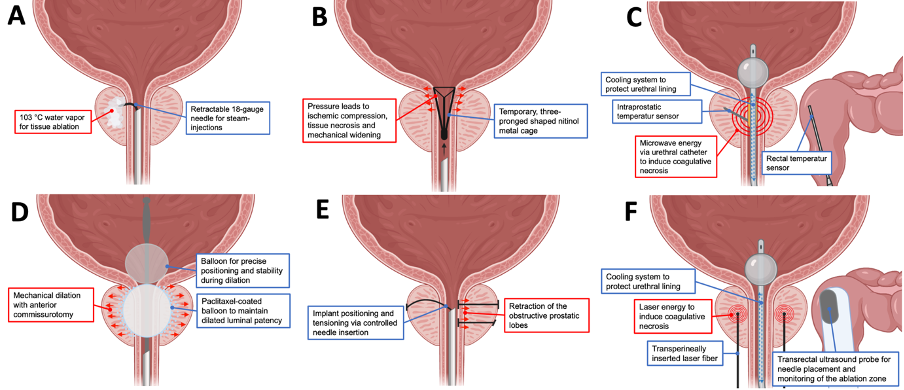
Schematic illustration of minimally invasive surgical therapies for benign prostatic obstruction. (A) Rezūm, (B) iTind, (C) CoreTherm, (D) Optilume BPH, (E) UroLift, (F) Echolaser.
Comprehensive overview of minimally invasive surgical therapies for benign prostatic hyperplasia (BPH), summarizing perioperative requirements, clinical efficacy outcomes, and sexual function results. IPSS - International Prostate Symptom Score, Qmax - Peak urinary flow rate, QoL - Quality of life
|
Treatment Modality |
Minimal anesthesia required |
Postoperative catheter required |
Median lobe (obstructive) eligible |
Mean IPSS improvement at 12 months |
Mean Qmax change at 12 months (mL/s) |
Mean QoL Score change at 12 months |
Available follow-up |
Medical retreatment rate |
Surgical retreatment rate |
Erectile Function |
Ejaculatory Function |
|
Rezum |
Local ± sedation |
Yes (3–5 days) |
Yes |
-8 to -13.5 |
+5 to +12 |
-2.1 to -3.1 |
5 years |
11% at 5 years |
2.5% at 1 year, 4.4% at 5 years |
Preserved |
3.2-3.6% anejaculation |
|
iTind |
Local ± sedation |
No |
No |
-9 to -13 |
+3.5 to +7.5 |
-1.9 to -2.4 |
4+ years |
2.4-4.7% at 1 year |
2.4-4.7% at 1 year, 8.6% at 3 years, 11% at 4+ years |
Preserved |
Preserved |
|
CoreTherm |
Local ± sedation |
Yes (5–7 days) |
No |
-12 to -15 |
+6 to +11 |
-2.7 to -3.1 |
5+ years |
Poorly reported; 1 study reported 2% after 5 years |
0-16.7% at 1 year, 5-20% at 3 years, 8-23% at 5 years |
7.5-8% impotence |
24-27% anejaculation |
|
Optilume BPH |
Local or general |
Yes (2-3 days) |
No data available |
-11.5 to -14.5 |
+7 to +10 |
-2.4 to -3.3 |
4 years |
4% combined retreatment rate at 1 year |
Preserved |
||
|
UroLift |
Local ± sedation |
Sometimes |
Yes |
-8.5 to -12.5 |
+2.5 to +6.5 |
-2.0 to -3 |
5 years |
3.6% at 1 year, 10.7% at 5 years |
2-6.9% at 1 year, 11% at 3 years, 13.6%% at 5 years |
Preserved |
Preserved |
|
TPLA (Echolaser) |
Local ± sedation |
Yes (1–3 weeks) |
Yes |
-8 to -13.5 |
+3 to +8.5 |
-2.6 to -3.7 |
4+ years |
0-17.5% at 1 year, 42.5% at 3 years, 37.5% at 57 months |
0-9% at 1 year |
Preserved |
1.2–15% anejaculation |
|
12.5% combined retreatment rate at 57 months |
|||||||||||
In addition to these established modalities, a new generation of stent-based First-line Interventional Therapies (FITs), including Zenflow, Butterfly, ProVerum, Urocross, and FloStent, has emerged. These systems are designed for office-based deployment under local anesthesia, offering immediate relief of obstruction with minimal recovery time and the flexibility of device retrieval or future treatment. Early clinical data show promising safety and efficacy profiles, underscoring their potential as a bridge or alternative to pharmacological or surgical therapy.
Taken together, MISTs now provide a wide therapeutic spectrum that can be tailored to individual patient anatomy, comorbidity, and treatment preferences. Across modalities, the ability to perform these procedures under local anesthesia, preserve sexual function, and offer rapid recovery is transforming patient expectations and redefining the treatment algorithm for BPO. As evidence continues to accumulate, further refinement of patient selection criteria and long-term outcome data will be essential to optimize their role in contemporary practice.
We believe that these function-preserving, office-based approaches will continue to complement and, for many men, replace conventional surgery, marking a decisive shift toward personalized and minimally invasive management of benign prostatic obstruction.
Written by: Nico C. Grossmann, MD, University Hospital Southampton NHS Trust, Southampton, United Kingdom; University Teaching and Research Hospital of the University of Lucerne, Lucerne, Switzerland
Read the Abstract