In this scenario, minimally invasive surgical therapies (MISTs) emerged as alternatives with the aim to reduce the overall rate of complications while maintaining efficacy. This systematic review evaluated the complication profiles of the mainly adopted MISTs—Aquablation, Rezūm, Transperineal Laser Ablation (TPLA), Prostatic Urethral Lift (PUL), and temporary implantable nitinol device (iTIND) to enhance the clinical decision-making process.
This review analyzed data from 24 studies involving 4,821 patients. In this light, Aquablation had the highest major complication rate (14%; IQR 6–22%), particularly in patients with prostate volumes over 80 mL, with bleeding and urethral strictures being the most reported issues. Rezūm demonstrated a lower major complication rate of 6.7%, though acute urinary retention (AUR) occurred in up to 8% of cases, especially in larger prostates. TPLA showed a favorable safety profile, with complication rates up to 13%, primarily minor and short-term events like urinary retention and urinary tract infections. Similarly, PUL was associated with a mid-term retreatment rate of 10.9% but had a lower incidence of bleeding compared to TURP. iTIND had the lowest complication rates among MISTs, with few cases of device-related urinary retention requiring operative removal. Across all therapies, sexual function outcomes were better preserved compared to conventional treatments, further underscoring the advantages of MISTs.
While variability in complication rates reflects differences in technique, patient selection, and study methodologies, this review highlights the importance of individualized treatment strategies. Aquablation is more suited for larger prostates, while Rezūm and TPLA are safer options for smaller glands. PUL and iTIND, with lower risks and shorter recovery times, may benefit younger patients or those prioritizing minimal disruption.
These findings emphasize that MISTs offer a promising balance of safety and efficacy in managing BPH-related LUTS, providing viable alternatives to traditional approaches. Further high-quality, long-term studies are necessary to refine patient selection and optimize outcomes.
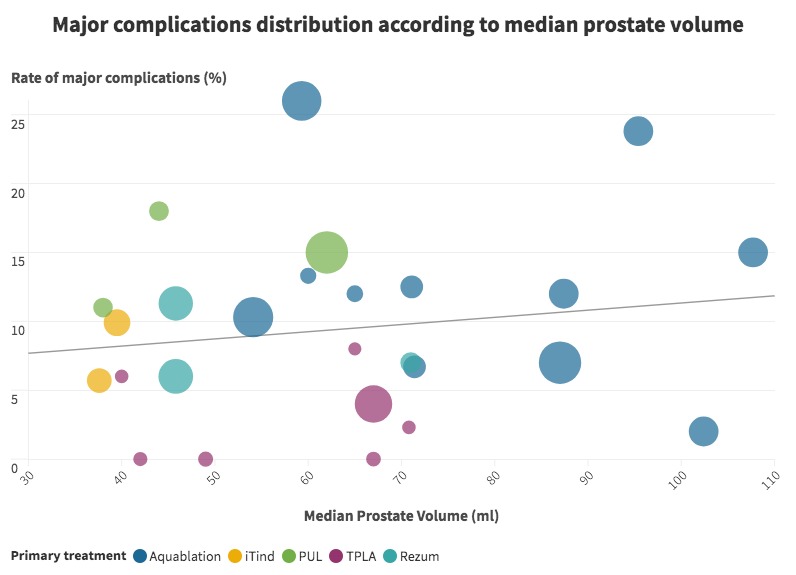
Figure 2 represents the distribution of major complications across the different minimally invasive techniques and series
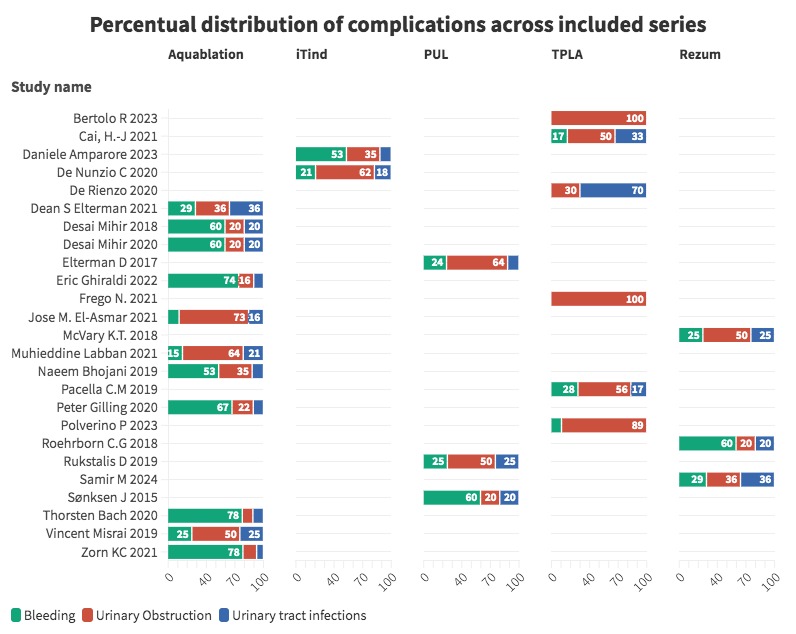
Figure 3 highlights the percentage of different kind of overall complications across the reported series.
Written by: Luca Lambertini,1 Alessandro Sandulli,1 Simone Coco,1 Daniele Paganelli,1 Anna Cadenar,1 Paolo Dell'Oglio,2 Stefano Puliatti,3 Fabrizio Di Maida,1 Antonio Andrea Grosso,1 Daniele Amparore,4 Riccardo Bertolo,5 Riccardo Campi,6 Riccardo Lombardo,7 Matteo Ferro,8 Bernardo Rocco,8 Gianni Vittori,1 Alessandro Antonelli,5 Cosimo De Nunzio,7 Andrea Minervini,1 Andrea Mari1
- Oncologic Minimally Invasive Urology and Andrology Unit, Department of Experimental and Clinical Medicine, Careggi Hospital, University of Florence, Florence, Italy.
- Department of Urology, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy.
- Department of Urology, University of Modena and Reggio Emilia, Modena, Italy.
- University of Turin San Luigi Gonzaga Hospital, Division of Urology, Turin, Italy.
- Department of Urology, University of Verona, Azienda Ospedaliera Universitaria Integrata, Verona, Italy.
- Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy; Unit of Urological Robotic Surgery and Renal Transplantation, University of Florence, Careggi Hospital, Florence, Italy.
- Department of Urology, Sant'Andrea Hospital, Sapienza University, Rome, Italy.
- Unit of Urology, Department of Health Science, University of Milan, ASST Santi Paolo and Carlo, Milan, Italy.