In the past, radical prostatectomy (RP) was indicated for low risk patients and was associated with overtreatment with a limited survival benefit. At present, high risk patients may benefit the most from RP. There are currently more advanced technology, biomarkers and imaging modalities being used, assisting in diagnosis and treatment. The multimodal approach is much more commonly utilized. RP is evolving to an operation for higher grade and stage disease, involving more meticulous dissection to ensure negative margins, more extended lymph node dissection, and possible treatment of local and distant metastasis.
It is known that as the pathologic T stage worsens, the location of positive surgical margins (PSM) changes as well. It has also been shown that an increased extracapsular extension distance is correlated with higher risk for biochemical recurrence. The patients who are at risk for PSM include those with adverse genomics, patients with imaging showing PIRADS 5 lesion, and high CAPRA score (composed of age, PSA, Gleason score, disease grade and volume).
Dr. Caroll continued to discuss whether it is possible for us to achieve cancer control and maintain a good quality of life. Nerve preservation during RP is possible in high risk disease according to Dr. Carroll. However, the surgeon must be a high volume operator with considerable experience.
The controversial issue of whether pelvic lymph node dissection (PLND) is therapeutic was discussed next. There is a considerable number of studies addressing this issue with contradicting results. It is assumed that more extensive PLND improves survival in patients with node positive PC.
This topic lead to another contemporary controversial issue of treating oligometastatic disease (M1), defined as less than 5 metastases, bone or lymph node (excluding visceral metastasis). There are two related trends driving the M1 stage migration. These includes the rising use of advanced imaging with greater sensitivity (PSMA, Choline 11, Na-18F PET/CT/MRI), and the end of theraputical nihilism regarding the treatment of advanced disease. There are currently several ongoing prospective randomized controlled trials assessing the role of treatment in oligometastatic disease. One such study is the HORRAD trial, comparing standard hormonal treatment to standard hormonal treatment with local external radiotherapy in bone metastatic PC patients1 (Figure 1). Another similar study is the STAMPEDE trial comparing multiple arms of newly diagnosed metastatic patients, including hormonal treatment, radiation and the cokbination of abiraterone and enzalutamide1 (Figure 2).
There is a clear pattern change over the last few years, demonstrating that PC with rising CAPRA scores are more commonly being treated with RP (Figure 3). In summary, RP can be better defined using a multivariable risk model rather than simple operational definitions. It is a spectrum of disease which is being better defined using molecular and novel imaging tools. There is increasing evidence that more aggressive treatment, often in combination with additional treatments, will lead to better outcomes. Dr. Carrol concluded his great talk by recommending surgeons to track their outcomes, be transparent and enroll patients in clinical trials.
Figure 1 – Study design for the HORRAD trial:
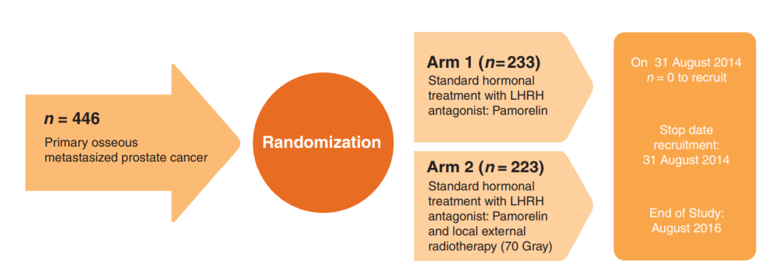
Figure 2 – Study design for the STAMPEDE trial:
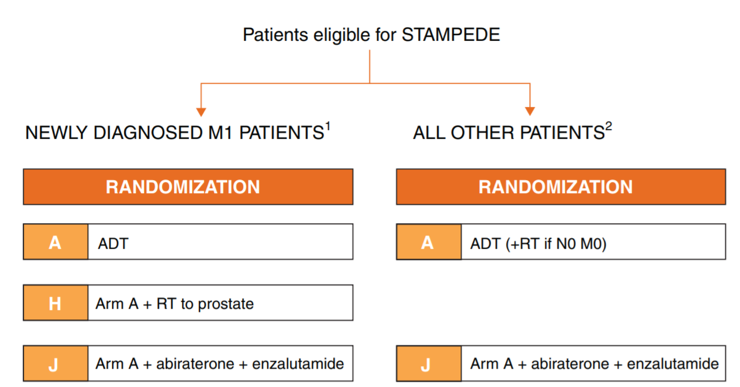
Figure 3 – Treatment of rising CAPRA score during the last years

Presented By: Peter Carroll, UCSF department of Urology, San Francisco, CA, USA
Written By: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre @GoldbergHanan at the 2018 North American Robotic Urology Symposium, February 16-17, 2018 - Las Vegas, NV
References:
1. Bayne CE, Williams SB, Cooperberg MR, et al. Treatment of the Primary Tumor in Metastatic Prostate Cancer: Current Concepts and Future Perspectives. European urology; 69(5): 775-87.