Focusing on The First and Only FDA Approved Targeted Alpha Therapy Radium-223 in the Treatment of mCRPC
The Tenth Symposium on Targeted Alpha Therapy (TAT-10) opened on Wednesday, May 31, 2017 in Kanazawa Japan. The symposium was jointly organized by the Joint Research Centre (JRC) of the European Commission and Kanazawa University as a forum for presentations on the latest developments in radiotherapy with alpha emitters in cancer. With over 200 participants the symposium covered advances in cancer treatment using alpha emitters as targeted therapy, clinical and preclinical research, radionuclide production, instrumentation and dosimetry.1
Four of the major alpha emitters radium-223, thorium-227, actinium-225, and astatine-211 will be discussed in this review that were presented during the TAT-10 Symposium. A significant milestone occurred for targeted alpha therapy when in 2013 radium-223 dichloride (radium-223) was approved by the FDA as the first in class and to date only targeted alpha therapy marketed as Xofigo®).2,3 The approval of radium-223 was a major step forward in the treatment of metastatic castration-resistant prostate cancer (mCRPC). The pivotal phase III ALSYMPCA (Alpharadin in the Treatment of Patients With Symptomatic Bone Metastases in Castration-Resistant Prostate Cancer) trial demonstrated statistically significant improvement in overall survival in patients with osseous metastasis. 4
CLINICAL UPDATE
Treating men with advanced prostate cancer involves consideration of how to treat each patient, when to treat and what treatment or combination of treatments to use and importantly what tests to use to assess the benefits of the selected treatment. In a retrospective study of heavily pre-treated population with a 64% one-year survival, patients with mCRPC had improved survival if they received radium-223 before being treated with cytotoxic chemotherapy when they had elevated baseline serum alkaline phosphatase (ALP). What emerges from this and other prospective studies is the importance of using radium-223 earlier in the patient’s disease when patients are more likely to receive the six planned cycles.5
Following the ALSYMPCA trial the patients were enrolled in an international, early access program (iEAP), open-label, single-arm phase 3b trial.6 The purpose was to see if there were significant differences in asymptomatic patients at baseline compared to symptomatic patients for early treatment with radium-223. Asymptomatic was defined as no pain and no opioid use. Patients were excluded if they had malignant lymphadenopathy > 6 cm and visceral disease.6
Asymptomatic patients had received fewer prior treatments of abiraterone, enzalutamide, and docetaxel, and were more likely to complete the full treatment of 6 cycles of radium-223. Adverse events were less common in asymptomatic patients. Asymptomatic patients were more likely to show alkaline phosphatase (ALP) normalization (59% vs 34%).7 Looking for candidates assessing efficacy for radium-223, an exploratory analysis of iEAP data revealed that ALP was a candidate for a biomarker of disease status. Median overall survival was longer in asymptomatic patients (median 20.5 months vs 13.5 months for symptomatic). Median overall survival was also longer in patients who received radium-223 plus abiraterone, enzalutamide, or both than in those who did not receive these agents. Similarly overall survival was longer in patients who received radium-223 plus docetaxel than in patients who received radium-223 without docetaxel.7,8
The investigators concluded that radium-223 can be safely combined with abiraterone or enzalutamide.6 A decline in alkaline phosphatase was associated with longer overall survival, and time to first symptomatic skeletal events (SSE).7 Patients who were asymptomatic, no pain and no opioid use at baseline, were more likely to have a better prognosis and to complete all 6 cycles of radium-223. 8
Consequently, the treatment paradigm is shifting from what was the standard of care 9 to therapeutic layering 10 in mCRPC with immunotherapy – targeted alpha radium therapy – chemotherapy on top of continuing second generation androgen pathway inhibitors, traditional androgen-deprivation therapy, and best supportive care when further treatments will not improve survival.6 Timing of delivering each treatment is critical. Treating early, before symptoms of pain develop from metastatic disease and monitoring markers of disease progression, then layering therapies is demonstrated to improve overall survival and quality of life.
BACKGROUND TO RADIATION
The use of radiation in medicine has a long history starting in the late nineteenth century with the notable discovery of radium by Marie Curie. The major types of ionizing radiation emitted during radioactive decay are alpha particles, beta particles and gamma rays [Figure 1]. 11,12,13
Figure 1: Alpha Particle Decay
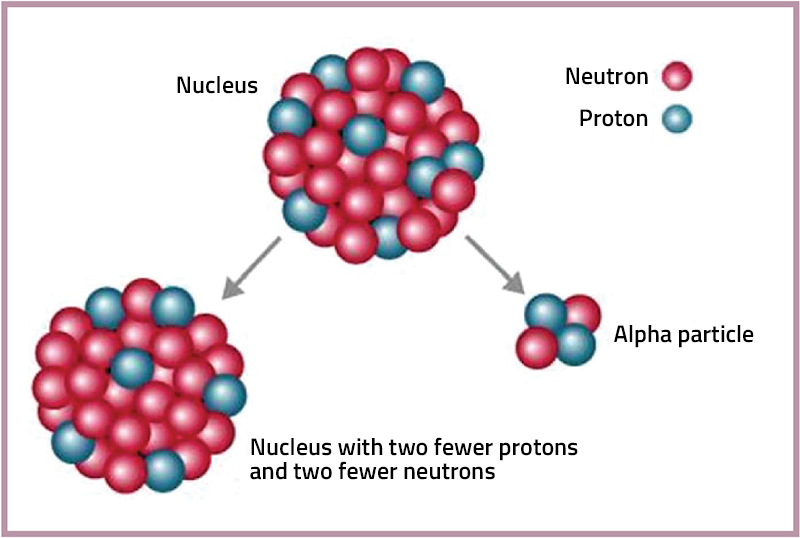
An alpha particle consists of two protons and two neutrons, the equivalent of a helium nucleus. Alpha particles are emitted from the decay of certain heavy radioactive nuclei, such as uranium, actinium and radium. They are very energetic and highly ionizing, i.e. short range (0.1 mm); high energy loss (50 - 230 keV/micrometer). The much high linear energy transfer (LET) causes irreparable damage to the cell DNA while the short range of the alpha confines the damage to the tumor thus reducing the damage to nearby healthy cells. External bodily exposure carries little risk to health, however, if inhaled or ingested, alpha particles can cause severe damage at both cellular and genetic level. This makes alpha particles possibly the most damaging form of radiation.11,12, 13
Beta-emitters have a relatively long radiation range and significant bone marrow exposure is associated with their use which has restricted bone treatment to pain palliation.14 Beta particles are electrons (or positrons) emitted from certain nuclei during radioactive decay. They have longer range (110 millimeters) and lower linear energy transfer (0.2keV/micrometer) than alpha particles. To cause irreversible DNA damage and induce cell death beta particles require 102–103 tracks across a section of DNA, whereas alpha-particles require only 2–3 tracks. Common beta emitters include carbon-14 and strontium-90.11, 12
Terminology may be confusing. Measurements of radiation dose are given in Curies and/or Bequerels. Curie (Ci) is the traditional measure of radioactivity based on the observed decay rate of 1 gram of radium. One curie of radioactive material will have 37 billion disintegrations in 1 second. It has been replaced by the term Becquerel (Bq), the amount of a radioactive material that will undergo one decay (disintegration) per second.13,15
Some of the commonly used terms to quantify radiation are radioactivity, exposure, effective dose, and absorbed dose. Radioactivity is the amount of ionizing radiation released by a material. Exposure measures the amount of radioactivity traveling through the air. Absorbed dose describes the amount of radiation absorbed by an object or person. The most common unit of measure for this is the Gray (Gy), where one Gray is equivalent to one Joule per kilogram in the international system (SI) unit of radiation dose. The Gray (Gy) has replaced the term rad, and one Gray equals 100 rad. Effective dose combines the absorbed dose and the medical effects of the type of radiation. For beta and gamma radiation the Effective Dose (expressed in Sievert (Sv) is equivalent to the absorbed dose. For alpha radiation which is more damaging to the body, the Effective Dose may be greater.11
When reading “Dosage and Administration” of the Package Insert for radium-223, the instructions are in both the newer and the older terms. The recommended dose of radium-223 is 55 kBq (1.49 microcurie) per kg body weight, given at 4 week intervals for 6 injections.3
UNIQUE PROPERTIES OF RADIUM-223
Radium-223 is a bone-targeting radiopharmaceutical and can substitute for calcium during bone formation. It belongs to the same group in the Periodic Table of the Elements as alkaline earth elements (calcium (Ca), strontium (Sr), barium (Ba), and radium (Ra)) and has similar bone seeking properties.
Radium-223 is easily administered directly into the bloodstream.3 It is a calcium mimetic and as long as the target is calcium, radium-223 is its own vector. This characteristic puts radium-223 in a special category. 14 It homes to bone and bone metastases where it can do its nefarious work in the tumors. It delivers an intense and highly localized radiation dose (with a range of 2 to 10 cell diameters) to bone surfaces. The higher LET of alpha-particles leads to a higher fraction of double strand breaks than with either beta-particles and gamma irradiation and leads to greater biological effectiveness. The cell is less able to repair DNA double strand breaks than single strand breaks. The number of DNA hits needed to kill a cell with an alpha particle is fewer than with beta emitters.14, 16,17 Moreover, radium-223 does not require cells to cycle in order to achieve its antitumor effect. This is advantageous in the treatment of prostate cancer, which has a low proliferative rate.18
Radium-223 decays to daughters, spontaneously breaking down to release energy and matter from its nucleus. Together with its daughters (three of which are also alpha emitters) radium-223 is even more potent, causing double-stranded DNA breaks leading to cell death.19 These characteristics represent hope for patients with CRPC and bone metastases. Targeted alpha therapy has the potential to inhibit the growth of micrometastases by selectively killing bone-derived cancer cells.
OTHER ALPHA EMITTERS FOR THERAPY
Several alpha-particle emitters with suitable half-lives are currently in use or being investigated for use in human trials: astatine-211 (211At, 7.2 h), bismuth-212 (212Bi, 1 h), bismuth-213 (213Bi, 45.6 min), radium-223 (223Ra, 11.4 d), actinium-225 (225Ac, 10.0 d) and thorium-227 (227Th, 18.7 d).
Different from radium-223 which homes to bone naturally, other alpha emitting elements require a molecular vector to attach to the tumor of interest and to carry the alpha-emitting radionuclide. Generally the form for delivery to a tumor cell consist of an antibody to a tumor surface antigen, attached to chelator and then to the alpha emitter. The alpha particle delivering structure is similar to a “sandwich” consisting of an antibody that attaches directly to an antigen in the tumor or on its surface, a chelating agent which acts as a linker to join the antibody to the radioisotope. Alpha emitters constructed for delivery can attack various tumor types in many locations, weeding out micrometastases. The vector combines the sciences of biology, chemistry and physics.26
Innovations galore were presented describing potential choices of the three components depending on the tumor of interest. The parameters that drive the choices include pharmacokinetics of the vector, the availability and half-life of the radioisotope, and the specificity of the vector to prevent accumulation in non-targeted organs.
There is a complication to this vector-targeting scheme. When the first alpha-emitting decay occurs, the recoil of the daughter nucleus is sometimes sufficient to break the molecular bond holding the radionuclide and the daughters are no longer bound to the tumor site [Figure 2]. Long-lived daughters can move through the body removing subsequent alphas from the tumor site and possibly damaging healthy organs, especially the liver and kidneys.3, 20
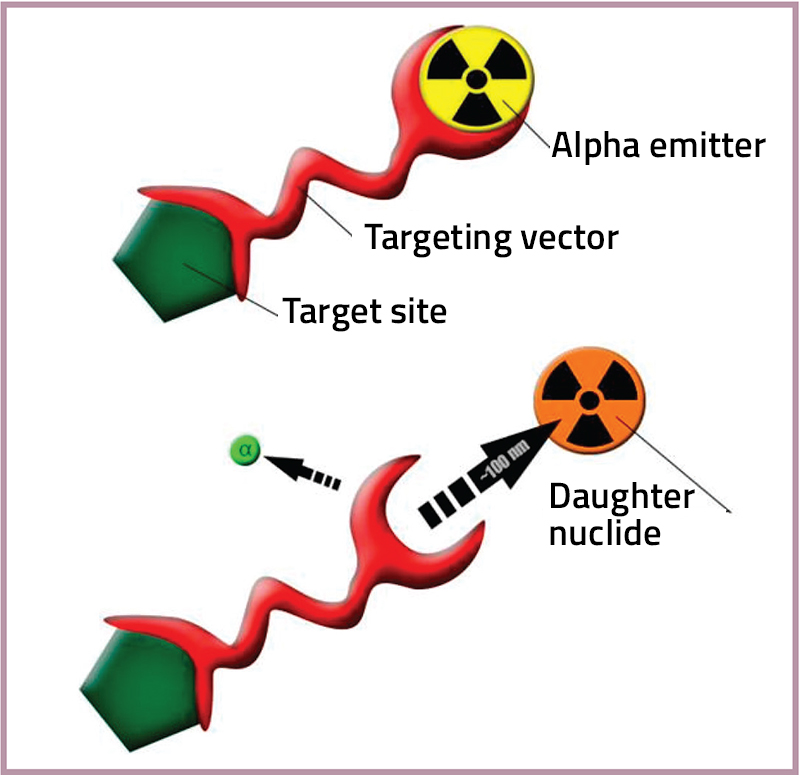
Figure 2: This illustration characterizes the targeting vector and a schematic representation of a recoiling daughter radionuclide detaching from a targeting agent as a consequence of alpa decay. 19
TO TAME THE DAUGHTERS
The main objective of targeted radionuclide therapy is the ability to selectively deliver cytotoxic radiation to cancer cells that cause minimal toxicity to the surrounding healthy tissues. Utilization of appropriate carriers capable of retaining both the parent and the daughter products for the effective delivery of the radionuclide to the tumor site, while mitigating global in vivo radiotoxicity is an active area of research. The use of nanoparticles for this purpose was very much in evidence at the meeting. The one potentially effective carrier of radium isotopes is a lanthanum phosphate core surrounded by nanoparticles to hold the radionuclide and retain the parents and daughters. 20 Investigation of this construct 22 and other nanoparticles as carriers such as gold 23, polymersomes 24 and others 25 were presented.
One innovative choice for the antibody part of the vector is the nanobody, the smallest, antigen-binding fragment from naturally occurring heavy-chain only antibodies. Nanobodies possess various advantages over monoclonal antibodies. The molecular weight of nanobodies (15 kDa) is one-tenth of that of conventional antibodies (150 kDa). Therefore, they have a lower immunogenicity due to their rapid blood clearance and high sequence identity to human variable domains of the heavy chain. Nanobodies are easy to produce and have high stability in harsh conditions, as well high affinity and specificity for their cognate antigen. 27 Several have been evaluated in pre-clinical studies.28,29
THE SHORT-LIVED ALPHA-EMITTERS, 211AT AND 213BI
Innovations galore were presented describing potential choices of the three components depending on the tumor of interest. The parameters that drive the choices include pharmacokinetics of the vector, the availability and half-life of the radioisotope, and the specificity of the vector to prevent accumulation in non-targeted organs.
There is a complication to this vector-targeting scheme. When the first alpha-emitting decay occurs, the recoil of the daughter nucleus is sometimes sufficient to break the molecular bond holding the radionuclide and the daughters are no longer bound to the tumor site [Figure 2]. Long-lived daughters can move through the body removing subsequent alphas from the tumor site and possibly damaging healthy organs, especially the liver and kidneys.3, 20
Figure 2: This illustration characterizes the targeting vector and a schematic representation of a recoiling daughter radionuclide detaching from a targeting agent as a consequence of alpa decay. 19
TO TAME THE DAUGHTERS
The main objective of targeted radionuclide therapy is the ability to selectively deliver cytotoxic radiation to cancer cells that cause minimal toxicity to the surrounding healthy tissues. Utilization of appropriate carriers capable of retaining both the parent and the daughter products for the effective delivery of the radionuclide to the tumor site, while mitigating global in vivo radiotoxicity is an active area of research. The use of nanoparticles for this purpose was very much in evidence at the meeting. The one potentially effective carrier of radium isotopes is a lanthanum phosphate core surrounded by nanoparticles to hold the radionuclide and retain the parents and daughters. 20 Investigation of this construct 22 and other nanoparticles as carriers such as gold 23, polymersomes 24 and others 25 were presented.
One innovative choice for the antibody part of the vector is the nanobody, the smallest, antigen-binding fragment from naturally occurring heavy-chain only antibodies. Nanobodies possess various advantages over monoclonal antibodies. The molecular weight of nanobodies (15 kDa) is one-tenth of that of conventional antibodies (150 kDa). Therefore, they have a lower immunogenicity due to their rapid blood clearance and high sequence identity to human variable domains of the heavy chain. Nanobodies are easy to produce and have high stability in harsh conditions, as well high affinity and specificity for their cognate antigen. 27 Several have been evaluated in pre-clinical studies.28,29
THE SHORT-LIVED ALPHA-EMITTERS, 211AT AND 213BI
The short-lived alpha-emitters, 211-astatine and 213-bismuth, may have potential as radioimmunotherapeutics in humans. Bismuth-213 has the disadvantage of a very short, 46 minute, half-life which usually requires direct injection into the tumor site.
Astatine-211 is an alpha-emitting halogen and has an acceptable half-life for cancer therapy (half-life =7.2 h). However, many astatine compounds that have been synthesized are unstable in vivo, providing motivation for seeking other astatine-211 labeling strategies. Most of the currently labelling protocols are developed based on iodine chemistry and lead to the formation of astatobenzoate-labelled compounds. Such labelling is unstable, contrary to the iodine case, when the carrier molecule is metabolized. Its limited availability and poorly known basic chemistry hamper the development of specific protocols for astatine-211. 30 Exploration of the fundamental chemistry of astatine is ongoing.31 Research on the chemistry of astatine effort is focused on optimizing attachment to antibodies 32 and assuring that the constructs comply with Good Manufacturing Practices.33
LONGER-LIVED ALPHA EMITTERS
Astatine-211 is an alpha-emitting halogen and has an acceptable half-life for cancer therapy (half-life =7.2 h). However, many astatine compounds that have been synthesized are unstable in vivo, providing motivation for seeking other astatine-211 labeling strategies. Most of the currently labelling protocols are developed based on iodine chemistry and lead to the formation of astatobenzoate-labelled compounds. Such labelling is unstable, contrary to the iodine case, when the carrier molecule is metabolized. Its limited availability and poorly known basic chemistry hamper the development of specific protocols for astatine-211. 30 Exploration of the fundamental chemistry of astatine is ongoing.31 Research on the chemistry of astatine effort is focused on optimizing attachment to antibodies 32 and assuring that the constructs comply with Good Manufacturing Practices.33
LONGER-LIVED ALPHA EMITTERS
The longer-lived alpha emitters, radium-223 (11.4 d), actinium-225 (10.0 d) and thorium-227 (18.7 d) are suitable for clinical use. Thorium-227 is and alpha emitting radionuclide with a half-life of 18.7 days. Thorium-227 decays to radium-223 and other short-lived radionuclides in its decay chain to stable lead-207.
Investigations in mice show lymphocyte surface antigen CD70 to be a promising target for B-cell lymphomas and several solid cancers including renal cell carcinoma. Cell surface receptor CD70 targeted thorium-227 conjugate (CD70-TTC) is comprised of three components, a CD70 targeting antibody, a chelator moiety and the short-range, high-energy alpha-emitting radionuclide thorium-227. The conjugate showed dose dependent accumulation and growth inhibition in tumor cells.34
Thorium is co-produced with radium 223, and as with all the radionuclides improvements in purification and isolation are continuously being pursued.35 - 39, as well as targeted thorium conjugates suitable for pharmaceuticals.40
Actinium-225, an alpha emitter with a 10 day half-life, has had a substantial amount of non-clinical work to indicate that actinium attached to appropriate antibodies and linker molecules has therapeutic potential to treat metastatic breast cancer, and bladder cancer. Actinium-225 conjugated to prostate specific membrane antigen (PSMA) shows promise but long-term toxicity studies in mice indicated that late radiation nephropathy was a dose-limiting toxicity. 41 When the PSMA conjugated construct was tested in patients with mCRPC side effects to the salivary glands were problematic.42
Early clinical studies showed potential for actinium-225 in glioblastoma multiforme43 and acute myeloid leukemia.44 Efficacy of actinium-225-labeled anti-CD33 antibody in acute myeloid leukemia and can be correlated with peripheral blast count.44
Importantly, radionuclides are difficult to obtain and difficult to purify. Investigators are constantly making improvements to isolation and purification technologies. Many presentations discussed these issues. 45 - 53

Figure 3: Radium-223 - First in Class FDA Approved Targeted Alpha Therapy (TAT) - with Demonstrated Overall Survival Benefit in Prostate Cancer 56
SUMMING-UP
Investigations in mice show lymphocyte surface antigen CD70 to be a promising target for B-cell lymphomas and several solid cancers including renal cell carcinoma. Cell surface receptor CD70 targeted thorium-227 conjugate (CD70-TTC) is comprised of three components, a CD70 targeting antibody, a chelator moiety and the short-range, high-energy alpha-emitting radionuclide thorium-227. The conjugate showed dose dependent accumulation and growth inhibition in tumor cells.34
Thorium is co-produced with radium 223, and as with all the radionuclides improvements in purification and isolation are continuously being pursued.35 - 39, as well as targeted thorium conjugates suitable for pharmaceuticals.40
Actinium-225, an alpha emitter with a 10 day half-life, has had a substantial amount of non-clinical work to indicate that actinium attached to appropriate antibodies and linker molecules has therapeutic potential to treat metastatic breast cancer, and bladder cancer. Actinium-225 conjugated to prostate specific membrane antigen (PSMA) shows promise but long-term toxicity studies in mice indicated that late radiation nephropathy was a dose-limiting toxicity. 41 When the PSMA conjugated construct was tested in patients with mCRPC side effects to the salivary glands were problematic.42
Early clinical studies showed potential for actinium-225 in glioblastoma multiforme43 and acute myeloid leukemia.44 Efficacy of actinium-225-labeled anti-CD33 antibody in acute myeloid leukemia and can be correlated with peripheral blast count.44
Importantly, radionuclides are difficult to obtain and difficult to purify. Investigators are constantly making improvements to isolation and purification technologies. Many presentations discussed these issues. 45 - 53
Figure 3: Radium-223 - First in Class FDA Approved Targeted Alpha Therapy (TAT) - with Demonstrated Overall Survival Benefit in Prostate Cancer 56
SUMMING-UP
Current cancer treatment is rarely effective once the tumor has metastasized, and alpha-targeted therapy has focused on targeting metastatic spread. The eradication metastases requires a targeted therapy that is minimally susceptible to chemo- or radio-resistance, sufficiently potent to sterilize individual tumor cells and cell clusters and has acceptable toxicity. Targeted alpha-emitter therapy apparently meets these requirements. Current constraints are the lack of widespread availability of alpha-emitters, the physics, radiochemistry and radiobiological-expertise required for their clinical implementation, and concerns about potential toxicity.54
As we have seen at this meeting treatment is not an either/or decision. The actual picture is complicated, requiring careful evaluation of the patient and the available treatments. Layering treatments is the new paradigm. Timing is important too. The current standard treatment is to start treatment early. Treatment can start as soon as the disease progresses from asymptomatic to symptomatic mCRPC with immunotherapy to radium therapy to chemotherapy on top of continuing second generation androgen pathway inhibitors, traditional androgen-deprivation therapy, and best supportive care. Synergism amongst treatments frequently occurs.
Professor Joe O’Sullivan of Queen’s University, Belfast, Ireland delivered the lunch symposium summarizing bench to bedside for targeted alpha therapy. He remarked on the ever evolving treatment for mCRPC. Docetaxel is introduced at the outset concurrent with androgen deprivation therapy (ADT). If ADT fails and the mCRPC patient is asymptomatic, sipuleucel-T, abiraterone acetate, or enzalutamide can be added to the ADT therapeutic backbone. Hence the term therapeutic layering or layering therapy.10 As soon as the patient is mildly symptomatic, radium-223 is started and continued for 6 cycles.
New trials have shifted the paradigm again. They suggest adding abiraterone at the outset and continuing it in conjunction with radium-223 therapy.55 The implications of the changes in the therapeutic landscape are increased overall survival and challenges in current trial endpoints.
Other new therapies are poised to emerge from on-going trials. Actinium-225 conjugated to PMSA shows promise despite issues with side effects to be overcome. Thorium-227, the alpha-emitting parent of radium-223 theoretically could add another alpha to the tumor site. Pre-clinical studies are investigating various conjugates for thorium-227 including PSMA for prostate cancer.
The meeting ended on a positive note, calling for more personalized therapy and more ambitious treatment of mCRPC. What is becoming clear is that treatment decisions are not an either or process, but a careful evaluation of the patient in consideration of the patient’s singular case, stage of disease and attitude. Layering therapy uses all available treatments and keeps in mind how best to treat, not only in view of treatment but in consideration of stage of disease and timing of treatment. Radiation therapy will not replace chemotherapy, ADT and other standard care, but will be used as an optimal addition to prolong life and to improve quality of life. However, the total picture is much more complex than we hoped.
Written By: William C. Carithers, Jr., PhD
REFERENCES
2. National Cancer Institute (NCI). National Institutes of Health. https://www.cancer.gov/about-cancer/treatment/drugs/fda-radium-223-dichloride
3. Xofigo [package insert]. Whippany, NJ: Bayer HealthCare Pharmaceuticals Inc; 2013.
4. Parker C, Nilsson S, Heinrich D, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med 2013;369:213-223.
5. Alva A, Nordquist L, Daignault S, et al. Clinical correlates of benefit from radium-223 therapy in metastatic castration resistant prostate cancer. Prostate. 2017;77(5):479-488.
6. Saad F, Carles J, Gillessen S, et al. Radium-223 International Early Access Program Investigators. Radium-223 and concomitant therapies in patients with metastatic castration-resistant prostate cancer: an international, early access, open-label, single-arm phase 3b trial. Lancet Oncol. 2016 Sep;17(9):1306-1316.
7. Oyen W, Saad F, Gillessen S, et al. Heidenreich A et al. ,4 Daniel Keizman,5 Joe M. O’Sullivan,6 Joan Carles,7 Manfred Wirth,8 Kurt Miller,9 Giuseppe Procopio,10 Monica Seger,11 Sten Nilsson,12 Daniel Heinrich13. Changes in alkaline phosphatase (ALP) dynamics and overall survival (OS) in metastatic castration-resistant prostate cancer (mCRPC) patients treated with radium-223 in an international early access program (EAP). Proc TAT-10, p 27.
8. Oyen W, Saad F, Gillessen S, et al. Heinrich D et al.,4 DanielKeizman,5 Joe M. O’Sullivan,6 Joan Carles,7 Manfred Wirth,8 KurtMiller,9 Liping Huang,10 Monica Seger,10 Sten Nilsson,11 Axel. Heidenreich12. Radium-223 (Ra-223) in asymptomatic metastatic castration resistant prostate cancer (mCRPC) patients treated in an international early access program (iEAP). Proc TAT-10, p 28.
9. ASCO. Treatment of Metastatic Castration-Resistant Prostate Cancer. http://www.cancer.net/research-and-advocacy/asco-care-and-treatment-recommendations-patients/treatment-metastatic-castration-resistant-prostate-cancer
10. Donya M, Radford M, ElGuindy A, et al. Radiation in medicine: Origins, risks and aspirations, Global Cardiology Science and Practice 2014:57. http://dx.doi.org/10.5339/gcsp.2014.57
11. .Gudkov SV, Shilyagina NY, Zvyagin AV. Targeted Radionuclide Therapy of Human Tumors. Int J Mol Sci. 2015;17(1). pii: E33.
12. Primer on Radiation Measurement. Center for Disease Control. Accessed June 30, 2017 https://emergency.cdc.gov/radiation/glossary.asp#primer
13. Henriksen G, Breistøl K, Bruland ØS, et al. Significant antitumor effect from bone-seeking, alpha-particle-emitting (223)Ra demonstrated in an experimental skeletal metastases model. Cancer Res. 2002;62(11):3120-3125.
14. Allisy A. From the curie to the becquerel. Metrologia. 1995;32 (6):467–479.
15. Henriksen G, Fisher DR, Roeske JC, Bruland ØS, Larsen RH. Targeting of osseous sites with alpha-emitting 223Ra: comparison with the beta-emitter 89Sr in mice. J Nucl Med. 2003;Feb:44(2):252-259.
16. Graf F, Fahrer J, Maus S, et al. DNA double strand breaks as predictor of efficacy of the alpha-particle emitter Ac-225 and the electron emitter Lu-177 for somatostatin receptor targeted radiotherapy. PLoS ONE 2014; 9(2): e88239.
17. Cheetham PJ, Petrylak DP. Alpha particles as radiopharmaceuticals in the treatment of bone metastases: mechanism of action of radium-223 chloride (alpharadin) and radiation . Oncology (Williston Park). 2012;26(4):330-337.
18. Ritter MA, Cleaver JE, Tobias CA. High-LET radiations induce a large proportion of non-rejoining DNA breaks. Nature. 1977;266:653-655.
19. de Kruijff RM, Wolterbeek HT, Denkova AG. A critical review of alpha radionuclide therapy—how to deal with recoiling daughters? Pharmaceuticals 2015; 8: 321-336.
20. Rojas JV, Woodward JD, Chen N, et al. Synthesis and characterization of lanthanum phosphate nanoparticles as carriers for (223)Ra and (225)Ra for targeted alpha therapy. Nucl Med Biol. 2015; Jul;42(7):614-20.
21. Mirzadeh S, Rojas JV, McLaughlin MF, et al. WoodwardJD, et al.D. Robertson, and S. J. Kennel. Lanthanum phosphate nanoparticles as carriers for 225Ac, 223Ra and 225Ra for targeted alpha therapy. Proc TAT-10, p 48.
22. Koźmiński P, Janiszewska L, Pruszyński M, et al. Gold nanoparticle– conjugates as a carrier for 211At in alpha particle therapy. Proc TAT-10, p 50.
23. de Kruijff RM, Heskamp S, van der Meer A, et al. Assessing 225Ac-polymersomes for targeted radionuclide therapy.
24. Kozempel J, Vlk M, Mičolová P et al. Nanocarriers of 223Ra for targeted alpha therapy. Proc TAT-10, p 49.
25. Sofou S. Radionuclide carriers for targeting of cancer. Int. J Nanomedicine. 2008;3(2):181-199.
26. Dekempeneer Y, Keyaertsa M Krasniqia A, et al. Targeted alpha therapy using short-lived alpha-particles and the promise of nanobodies as targeting vehicle. Expert Opinion on Biological Therapy, 2016;16 (8):1035–1047.
27. Dekempeneer Y, D’Huyvetter M, Aneheim E, et al. Preclinical evaluation of astatinated nanobodies for targeted alpha therapy. Proc TAT-10, p 35.
28. Pruszyński N, D’Huyvetter M, Cędrowska E, et al. Preclinical evaluation of anti-HER2 2Rs15d nanobody labeled with 225Ac. Proc TAT-10, p.34.
29. Lindegren S, Palm S, Bäck T,et al. Realizing Clinical Trials with Astatine-211: Radiopharmaceutical Chemistry. Proc TAT-10, p 96.
30. Montavon G, Alliot C, Champion J, et al. Exploration of the chemistry of astatine; from basic research towards applied questions. Proc TAT-10, p 54.
31. Guérard F, Navarro L, Alliot C, et al. Progress in the [211At]-astatination of antibodies by nucleophilic approaches using aryliodonium salts precursors. Proc TAT-10, p 55.
32. Wilbur DS, Li Y, Hamlin DK, et al. Quality assurance and labeling chemistry qualification for cGMP production of astatine-211-labeled anti-CD45 antibodies. Proc TAT-10, p 56.
33. Hagemann UB, Mihaylova D, Uran SR, et al. Targeted alpha therapy using a novel CD70 targeted thorium-227 conjugate in in vitro and in vivo models of renal cell carcinoma. Oncotarget. 2017; Apr 7.
34. Frenvik JO, Dyrstad K, Kristensen S, Ryan OB. Development of separation technology for the removal of radium-223 from targeted thorium conjugate formulations. Part I: purification of decayed thorium-227 on cation exchange columns. Drug Dev Ind Pharm. 2017; Feb;43(2):225-233.
35. Frenvik JO, Dyrstad K, Kristensen S, Ryan OB. Development of separation technology for the removal of radium-223 from targeted thorium conjugate formulations. Part II: purification of targeted thorium conjugates on cation exchange columns. Drug Dev Ind Pharm. 2017 Sep;43(9):1440-1449.
36. Causey P, Bureau D, Leeder K, et al., Production of a thorium/actinium generator at the Canadian Nuclear Laboratories. Proc TAT-10, p 61.
37. Copping R, Birnbaum ER, Boll RA, et al. Chemical Purification of Actinium-225 from Proton-Irradiated Thorium Targets. Proc TAT-10, p 87.
38. Radchenko V, Baimukhanova A, Marinova A, et al. Behavior of Ac, Th and Ra on cation exchange resin in hydrochloric and trichloroacetic acids: Towards an alternative separation strategy for 225Ac from irradiated thorium targets. Proc TAT-10, p 88.
39. Ryan OB, Cuthbertson A, Herstad G, et al. Development of effective chelators for Th-227 to be used in Targeted Thorium Conjugates. Proc TAT-10, p 57.
40. Kratochwil C, Bruchertseifer F, Giesel FL, et al. 225Ac-PSMA-617 for PSMA-Targeted α-Radiation Therapy of Metastatic Castration-Resistant Prostate Cancer. J Nucl Med. 2016 Dec;57(12):1941-1944. Epub 2016 Jul 7.
41. Kratochwil C, Bruchertseife F, Giesel FL, et al. Ac-PSMA-617: PSMA targeting alpha-radiation therapy of patients with metastatic castration resistant prostate cancer (mCRPC). TAT-10, p 26.
42. Krolicki L, Bruchertseifer F, Kunikowska J, et al., Targeted alpha therapy of glioblastoma multiforme: clinical experience with 213Bi- and 225Ac-Substance P. Proc TAT-10, p24.
43. Berger M, Jurcic J, Scheinberg D. Efficacy of 225Ac-labeled anti-CD33 antibody in acute myeloid leukemia (AML) correlates with peripheral blast count. Proc TAT-10, p 22.
44. Alliot C, Bonraisin A-C, Audouin S, et al. Astatine-211 production using the C70XP. Proc TAT-10, p 100.
45. Causey P, Bureau D, Leeder K, et al Production of a Thorium/Actinium Generator at the Canadian Nuclear Laboratories. Proc TAT-10, 61.
46. Davern SM, O’Neil DW, Hallikainen H, et al. A novel micro-actinium 225-bismuth212 biomedical generator system. Proc TAT-10 p 59.
47. Harvey J, Kroc T. Progress toward an alternate method for production of Ac-225. Proc TAT-10, p 62.
48. John KD, Balkin ER, Birnbaum, ER, et al. US DOE Tri-Lab research effort to provide accelerator produced Ac225 for radiotherapy: 2017 update. Proc TAT-10, p 60.
49. O’Hara MJ, Krzysko AJ, Hamlin DK, et al. Laboratory automation employed in the purification of astatine-211 from dissolved bismuth targets: Development, optimization, and performance validation of the fluidic system. Proc TAT-10, p 95.
50. Pruszyński M, Cędrowska E, Bilewicz A et al. Radiochemical separation of 224Ra from 232U or 228Th sources for 224Ra/212Pb/212Bi generator. Proc TAT-10, p 89.
51. Shin Y, Ooe S, Murakami K, et al. Wet chemistry of radon and astatine for the development of a 211Rn/211At generator. Proc TAT-10, p 94.
52. Stein BW, Ferrier MG, Kozimor SA, et al. Spectroscopic and computational studies of actinium coordination chemistry. Proc TAT-10, p 58.
53. Sgouros G. 2009 Alpha-Particle Emitter Therapy: Overview, Current Status, and Dosimetry. Report on the Technical Meeting on Therapeutic Radiopharmaceuticals. http://www.iaea.org/inis/collection/NCLCollectionStore/_Public/43/005/43005466.pdf
54. Crawford ED, Petrylak DP, Shore N, et al. Prostate Cancer Radiographic Assessments for Detection of Advanced Recurrence (RADAR II) Group. The Role of Therapeutic Layering in Optimizing Treatment for Patients With Castration-resistant Prostate Cancer (Prostate Cancer Radiographic Assessments for Detection of Advanced Recurrence II). Urology. 2017;104:150-159.
55. Fizazi K, Tran N, Fein LE,et al. LATITUDE: Abiraterone plus prednisone in metastatic castration-sensitive prostate cancer. N Engl J Med. 2017 Jun 4. [Epub ahead of print
56. Phase I studies of Targeted thorium-227 conjugates are underway in Europe. *Progenics Pharmaceuticals Press Release May 2, 2016; **Kratochwil C et al. J Nucl Med 2016;57:1–4; #Currently in Phase 3, NCT02200614; §Currently in Phase 3, NCT02489318.