(UroToday.com) The 2025 Western Section AUA annual meeting featured a prostate cancer session and a presentation by Dr. David Crawford discussing PSA response with darolutamide + ADT in patients with metastatic hormone-sensitive prostate cancer in ARANOTE.1
In ARANOTE, darolutamide + ADT reduced the risk of radiological progression or death versus placebo + ADT by 46% in patients with metastatic hormone-sensitive prostate cancer (mHSPC). Notably, the incidence of treatment-emergent adverse events was low and similar between the groups. Patients achieving an undetectable PSA (< 0.2 ng/mL) at any time had a better ECOG performance status, lower Gleason score, and lower baseline PSA values versus those who did not. At the 2025 Western Section AUA annual meeting, Dr. Crawford and colleagues reported post-hoc analyses correlating PSA response with the outcomes overall and by baseline PSA level in ARANOTE.
Patients with mHSPC in ARANOTE were randomized 2:1 to darolutamide 600mg twice daily +ADT or placebo + ADT:
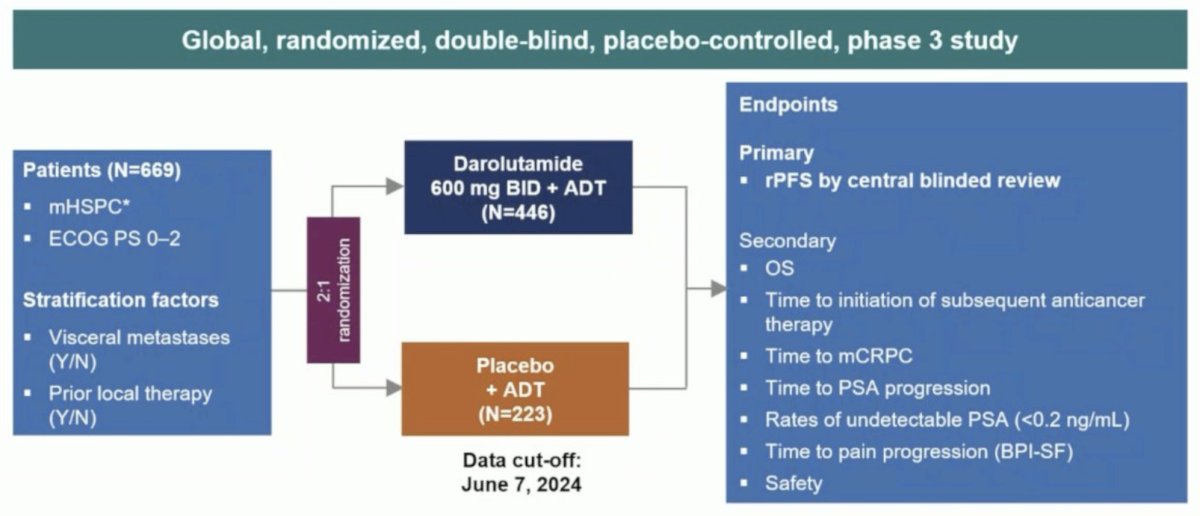
The achievement of undetectable PSA (<0.2 ng/mL) at any time was evaluated. Radiological progression free survival, time to metastatic castration resistant prostate cancer, and time to PSA progression were evaluated in patients who did and did not achieve PSA <0.2 ng/mL, and by baseline PSA group defined as <first quartile (Q1, <4.1 ng/mL), between Q1 and median (4.1–<21.3 ng/mL), and ≥median (≥21.3 ng/mL).
In 669 patients (darolutamide, 446 [67%]; placebo, 223 [33%]), more patients receiving darolutamide achieved PSA <0.2 ng/mL at any time (62.6%) versus placebo (18.5%):
![In 669 patients (darolutamide, 446 [67%]; placebo, 223 [33%]), more patients receiving darolutamide achieved PSA <0.2 ng/mL at any time (62.6%) versus placebo (18.5%):](/images/com-doc-importer/236-wsaua-2025/wsaua-2025-psa-response-with-darolutamide-adt-in-patients-with-metastatic-hormone-sensitive-prostate-cancer-in-aranote/image-1.jpg)
Patients receiving darolutamide who achieved PSA <0.2 ng/mL versus those who did not had a lower risk of radiological progression or death (81%, HR 0.19, 95% CI 0.13–0.27):

Patients receiving darolutamide who achieved PSA <0.2 ng/mL versus those who did not also had lower progression to metastatic castration resistant prostate cancer (84%, HR 0.16, 95% CI 0.12–0.23), and PSA progression (92%, HR 0.08, 95% CI 0.05–0.12). Regardless of baseline PSA group, more patients receiving darolutamide versus placebo achieved PSA <0.2 ng/mL at any time, with higher rates of PSA <0.2 ng/mL in patients with low baseline PSA (<4.1 ng/mL: darolutamide, 87.6% versus placebo, 43.5%; 4.1 to <21.3 ng/mL: 64.8% versus 14.0%; ≥21.3 ng/mL: 50.5% versus 10.2%):
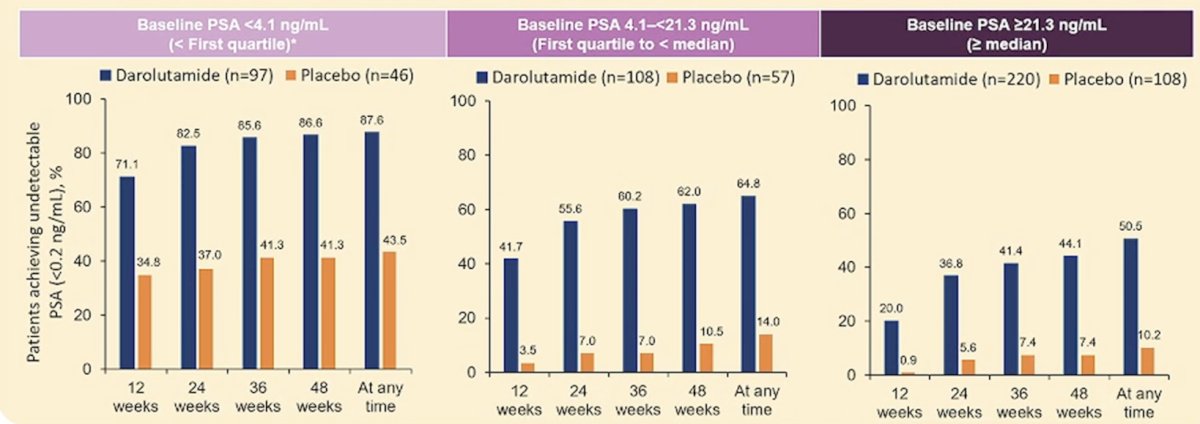
Patients receiving darolutamide with low baseline PSA (<4.1 ng/mL) had a longer time to radiological progression or death, time to metastatic castration resistant prostate cancer, and time to PSA progression versus patients with baseline PSA ≥21.3 ng/mL. The outcomes were also similar for patients with a baseline PSA of 4.1–<21.3 ng/mL versus ≥21.3 ng/mL. Safety with darolutamide was consistent with previous data and independent of PSA response/baseline PSA. Darolutamide showed lower rates of discontinuation due to treatment-emergent adverse events versus placebo.
Dr. Crawford concluded his presentation discussing PSA response with darolutamide + ADT in patients with metastatic hormone-sensitive prostate cancer in ARANOTE with the following take-home points:
- Darolutamide provided deep and durable responses in the overall population and across baseline PSA subgroups
- Three times as many patients reached an undetectable PSA (< 0.2 ng/mL) versus the placebo arm
- Undetectable PSA was achieved in a greater proportion of patients regardless of baseline PSA
- Undetectable PSA with darolutamide correlated with clinical benefit in terms of radiological progression or death, and longer time to mCRPC and PSA progression
- The safety profile of darolutamide was consistent across subgroups, regardless of PSA response and baseline PSA
Presented by: E. David Crawford, MD, Urologist, Professor of Urology, Jack A. Vickers Director of Prostate Cancer Research, University of California, San Diego, San Diego Health, San Diego, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Western Section American Urological Association (AUA) Annual Meeting, Napa Valley, CA, Sun, Nov 2 – Thurs, Nov 6, 2025.
Reference: